
Quick Answer
Pyometra is a life-threatening uterine infection in intact female dogs. This guide covers clinical signs distinguishing open from closed pyometra, emergency diagnostics, surgical spay as definitive treatment, and medical management with prostaglandin F2-alpha or aglepristone for breeding dogs.
Key Takeaways
- ✓Pyometra most commonly develops 2–8 weeks after estrus when progesterone promotes endometrial secretion and suppresses myometrial contractions, enabling E. coli colonization.
- ✓Closed pyometra carries higher risk for septic shock due to absence of drainage; these dogs deteriorate rapidly and require emergent surgical intervention.
- ✓Emergency OHE has a 90–95% cure rate in stable patients; always stabilize with IV fluids and broad-spectrum antibiotics before induction.
- ✓Prostaglandin F2-alpha (0.1 mg/kg SC SID x5–7 days) or aglepristone (10 mg/kg SC on days 1, 2, 8) are alternatives for stable breeding dogs with open-cervix pyometra.
- ✓PU/PD in pyometra is caused by E. coli endotoxin interfering with renal ADH receptors — not primary renal disease — and typically resolves post-treatment.
- ✓Any dog without clinical improvement within 48–72 hours of medical management should be converted to surgical treatment without further delay.
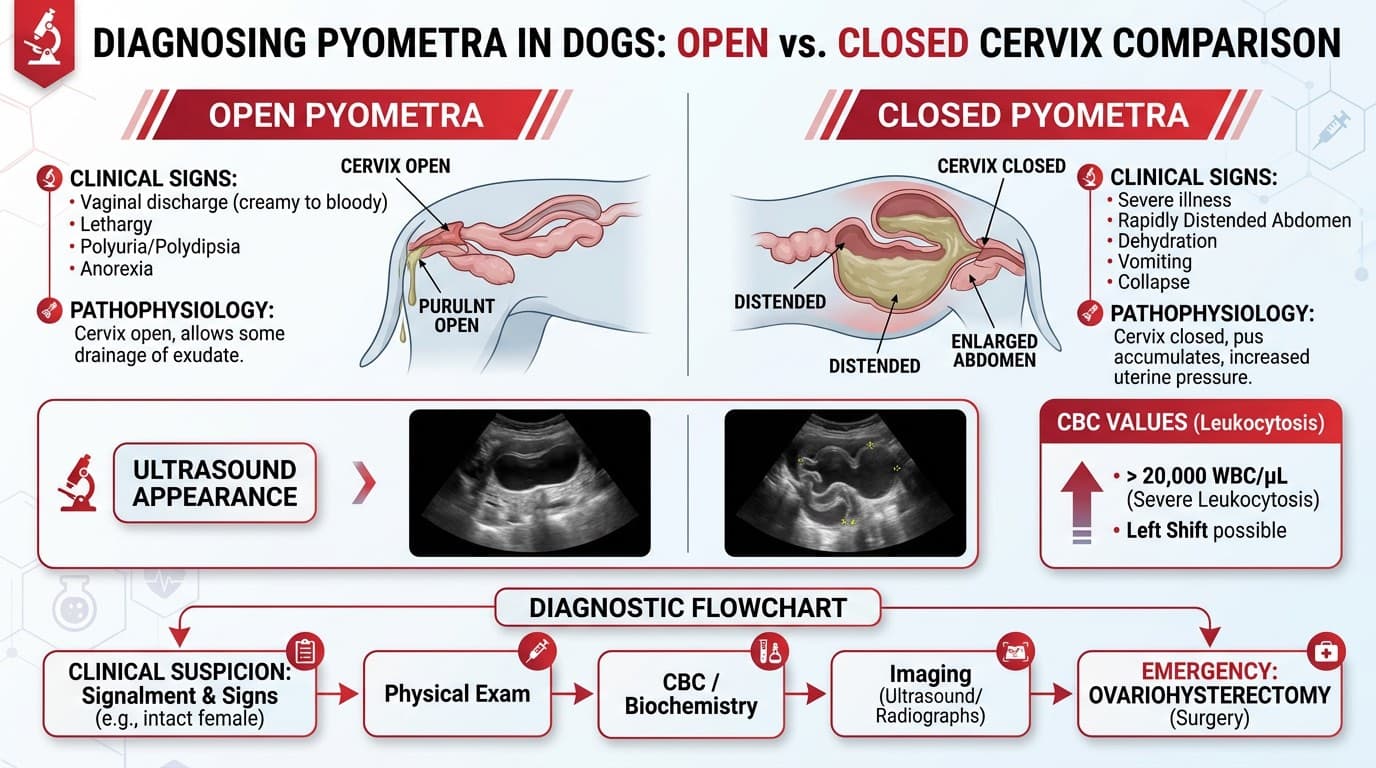
Open vs Closed Pyometra: Recognition and Emergency Diagnostics
Pyometra is a progesterone-driven bacterial infection of the uterus occurring in intact females, most commonly within 8 weeks of estrus. *Escherichia coli* accounts for approximately 70% of cases, colonizing the uterus via ascending vaginal contamination during diestrus when progesterone promotes endometrial gland secretion and suppresses myometrial contractions.
Classification
| Type | Cervix | Vaginal Discharge | Risk Level |
|---|---|---|---|
| Open pyometra | Open | Yes — mucopurulent, bloody, or malodorous | Moderate-high |
| Closed pyometra | Closed | No discharge | Critical — toxemia risk higher |
Clinical Signs
Common to both types:
- Polyuria/polydipsia (E. coli endotoxin interferes with renal tubular antidiuretic hormone response)
- Lethargy, anorexia
- Vomiting, mild abdominal distension
- History of estrus 2–8 weeks prior
Closed pyometra specifically: more acute systemic deterioration, septic shock, abdominal pain on palpation.
Emergency Diagnostics
| Test | Expected Finding |
|---|---|
| CBC | Leukocytosis >20,000/uL; left shift; toxic neutrophils |
| Chemistry | Elevated BUN/creatinine (prerenal or renal); elevated ALT; hypoglycemia in sepsis |
| Urinalysis | Isosthenuria (renal medullary washout from PU/PD); bacteriuria |
| Abdominal radiograph | Tubular soft tissue opacity displacing bowel; uterus >2 cm diameter |
| Abdominal ultrasound | Fluid-filled uterine horns; endometrial hyperplasia; may quantify fluid volume |
| Vaginal cytology | Degenerate neutrophils, intracellular bacteria in open cases |
Minimum Database Before Surgery Always obtain CBC, chemistry, and urinalysis before anesthesia induction. Correct dehydration and electrolyte imbalances (especially hypokalemia from vomiting) prior to induction when clinically feasible.
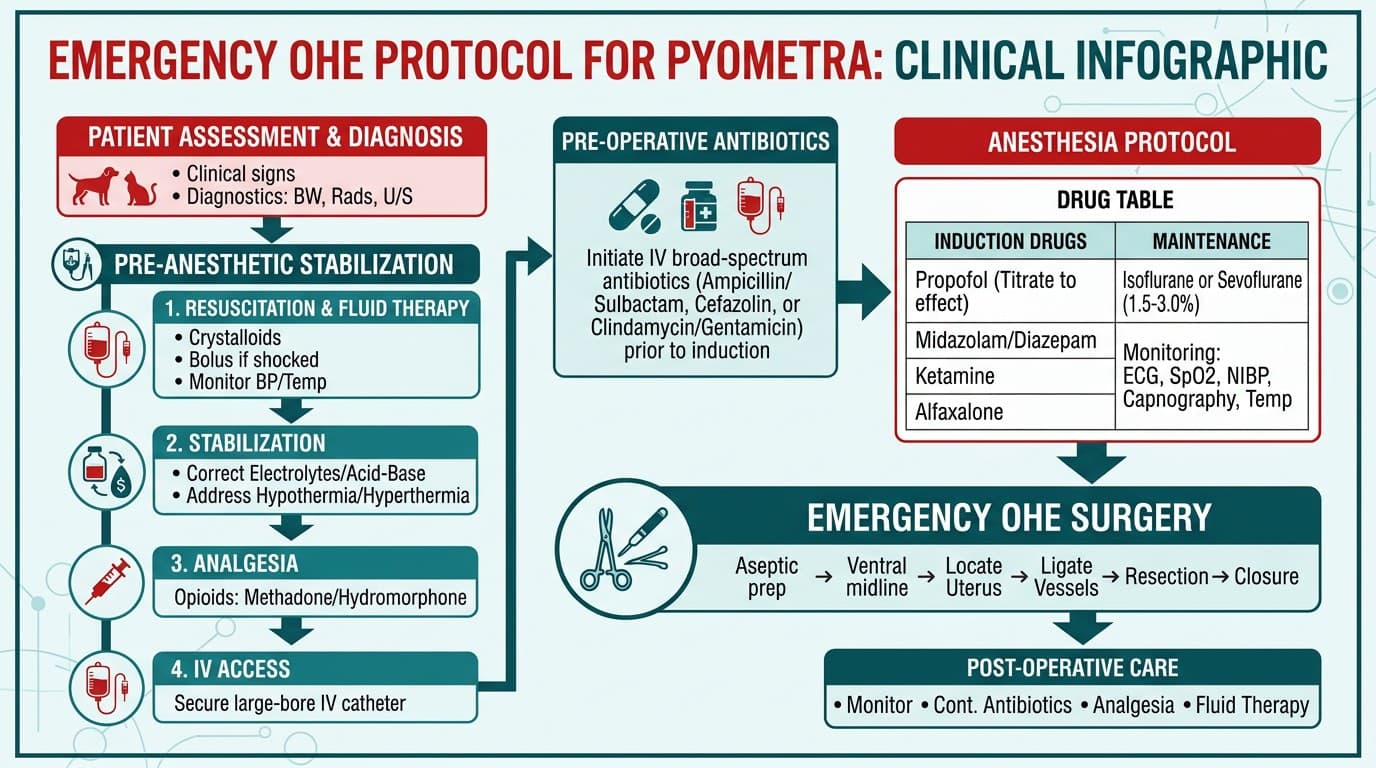
Emergency Ovariohysterectomy: Anesthesia and Surgical Protocol
Ovariohysterectomy (OHE) is the definitive and safest treatment for pyometra in most dogs. Cure rate exceeds 90% when performed before septic shock develops.
Pre-Anesthetic Stabilization
Target stabilization within 2–4 hours before induction when the patient is systemically compromised:
- IV catheter placement; crystalloid bolus 10–20 mL/kg over 15–30 minutes for hypovolemia
- Broad-spectrum IV antibiotics: amoxicillin-clavulanate 12.5 mg/kg IV BID + enrofloxacin 5 mg/kg IV SID or ampicillin-sulbactam 22 mg/kg IV TID
- Blood glucose monitoring; dextrose supplementation if <60 mg/dL
- Correct electrolyte derangements; supplement potassium in IV fluids if needed
Anesthesia Considerations
| Phase | Protocol |
|---|---|
| Pre-medication | Butorphanol 0.2–0.4 mg/kg IM + midazolam 0.2–0.4 mg/kg IM (opioid preferred over acepromazine in unstable patients) |
| Induction | Propofol 1–4 mg/kg IV (to effect); ketamine 2–5 mg/kg IV + midazolam 0.2 mg/kg IV if cardiovascular compromise |
| Maintenance | Isoflurane or sevoflurane in oxygen; reduce inhalant MAC with opioid CRI |
| Analgesia | Methadone 0.1–0.3 mg/kg IV or hydromorphone 0.1–0.2 mg/kg IV perioperatively |
Intraoperative Precautions
- Handle the uterus gently — avoid rupture and peritoneal contamination
- If uterus ruptures intraoperatively: copious lavage with warm sterile saline, culture uterine contents, prolonged antibiotic course
- Ensure both ovaries are completely removed to prevent stump pyometra
- Submit uterus for histopathology; culture uterine contents for organism identification
Post-Operative Care
- Continue IV antibiotics for 24–48 hours; then transition to oral amoxicillin-clavulanate 12.5–25 mg/kg PO BID for 7–10 days
- Monitor renal function with daily BUN/creatinine until values normalize
- Most dogs show dramatic clinical improvement within 24–48 hours of surgery
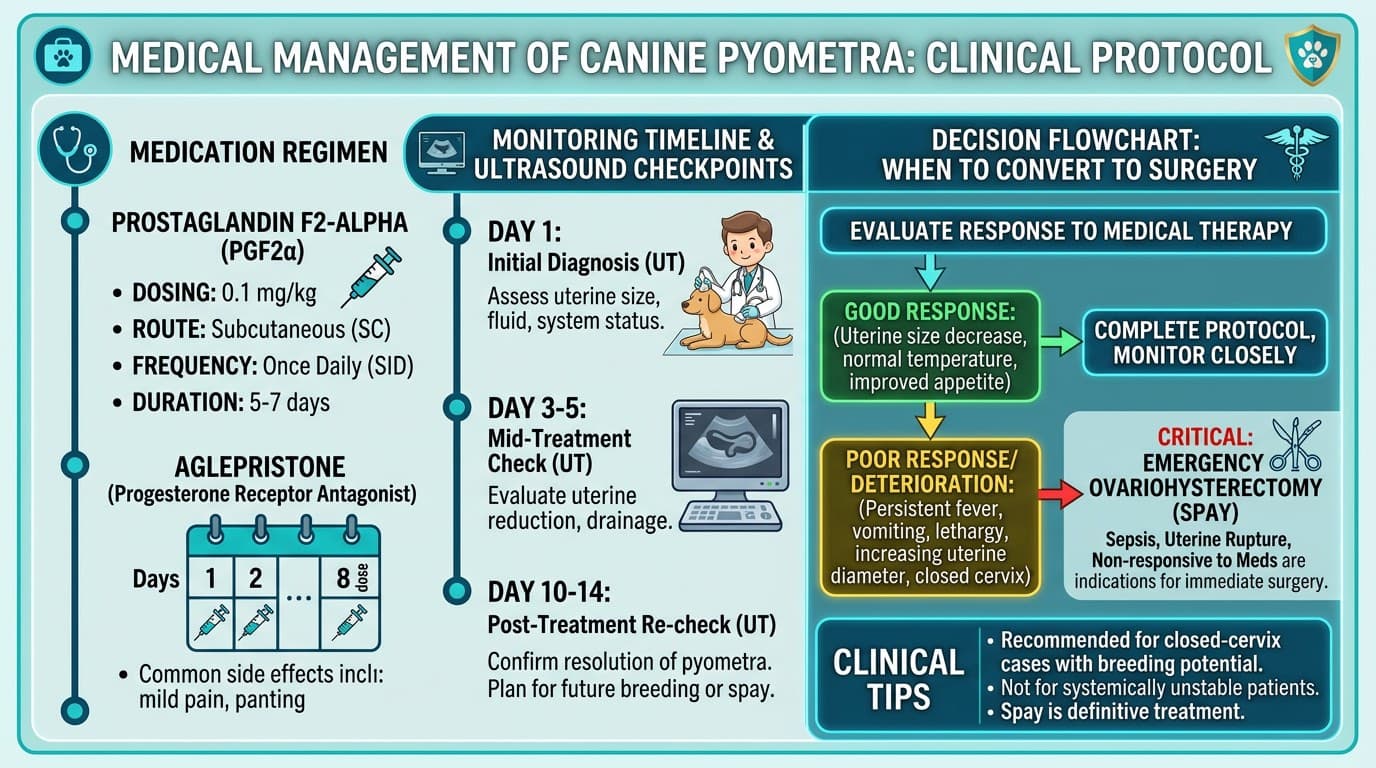
Medical Management for Breeding Dogs: Prostaglandins and Aglepristone
Medical management is reserved for open-cervix pyometra in stable breeding females where preserving fertility is a priority. Success rates are lower than surgery (approximately 70–90% for open pyometra with prostaglandins) and recurrence within the next heat cycle is common (25–40%).
Prostaglandin F2-alpha (Dinoprost Tromethamine — Lutalyse)
Mechanism: stimulates myometrial contractions and promotes cervical relaxation to expel uterine contents; also causes luteolysis, reducing progesterone.
| Parameter | Detail |
|---|---|
| Dose | 0.1 mg/kg SC SID (low-dose protocol) |
| Duration | 5–7 days until uterus decompressed on ultrasound |
| Side effects | Vomiting, defecation, panting, salivation within 30 min of injection (resolve in 1–2 hours); pre-treat with atropine 0.02 mg/kg SC to reduce severity |
| Contraindications | Closed pyometra, septic shock, significant azotemia, age <1 year |
Aglepristone (Alizin — available in Europe; compounded in USA)
Mechanism: progesterone receptor antagonist; blocks progesterone, opens cervix, allows uterine drainage.
| Parameter | Detail |
|---|---|
| Dose | 10 mg/kg SC on days 1, 2, 8 |
| Advantages | Fewer side effects than prostaglandins; can use in closed pyometra in some protocols |
| Combination | Aglepristone + cloprostenol (synthetic PGF2-alpha) improves success rates |
Antibiotic Coverage During Medical Management
- Start IV antibiotics immediately; transition to oral once drinking
- Recommended: amoxicillin-clavulanate 12.5 mg/kg PO BID throughout treatment
- Culture uterine discharge to guide targeted therapy
Monitoring
- Repeat abdominal ultrasound at days 5 and 14 to confirm uterine decompression
- Recheck CBC and chemistry at day 7
- Breed the dog on the NEXT heat cycle if fertility was the goal — do not delay surgery if improvement is not seen within 48–72 hours
When to Convert to Surgery
- No clinical improvement within 48–72 hours
- Development of signs of closed pyometra or septic shock
- Uterine rupture suspected
Frequently Asked Questions
How quickly does a dog with pyometra need surgery?
Closed pyometra is a critical emergency requiring surgery within hours. Open pyometra allows 2–4 hours for stabilization with IV fluids and antibiotics before induction. Do not delay surgery beyond 24 hours in any pyometra case.
Can pyometra be treated with antibiotics alone?
No. Antibiotics alone do not resolve pyometra because bacteria reside within the uterine lumen and the progesterone-primed environment continues to support infection. Antibiotics are used as adjuncts to surgical or prostaglandin-based treatment.
What is the survival rate for dogs with pyometra surgery?
Survival rate is 90–95% when surgery is performed before septic shock develops. Dogs in septic shock have a guarded prognosis with survival rates of 50–80% depending on severity and response to supportive care.
Can a dog get pyometra after being spayed?
Stump pyometra can occur if ovarian tissue is incompletely removed, leaving residual progesterone production. This is rare but presents identically to intact pyometra and requires surgical removal of the remnant ovarian tissue.
What is the recurrence rate after medical treatment of pyometra?
Recurrence within one or two subsequent estrous cycles occurs in 25–40% of dogs treated medically. Owners should be counseled to breed the dog on the very next cycle if fertility preservation was the treatment goal, then strongly consider OHE.
References
- Fransson BA, Lagerstedt AS, Hellmen E, Jonsson P. Bacteriological findings, blood chemistry profile and plasma endotoxin levels in bitches with pyometra or other uterine disease. J Vet Med A Physiol Pathol Clin Med. 1997;44(7):417-426.
- England GCW, Freeman SL, Russo M. Treatment of spontaneous pyometra in 22 bitches with a combination of cabergoline and cloprostenol. Vet Rec. 2007;160(9):293-296.
- Verstegen J, Dhaliwal G, Verstegen-Onclin K. Mucometra, cystic endometrial hyperplasia, and pyometra in the bitch: advances in treatment and assessment of future reproductive success. Theriogenology. 2008;70(3):364-374.