Quick Answer
Cryptorchidism is the most common canine reproductive disorder, affecting 1–3% of male dogs. This guide covers unilateral vs bilateral classification, abdominal and inguinal retention locations, markedly elevated cancer risk (Sertoli cell tumor, seminoma), and surgical orchidectomy approach selection.
Key Takeaways
- ✓Cryptorchidism affects 1–3% of male dogs with highest prevalence in toy breeds; right-sided abdominal retention is most common and carries the highest cancer risk.
- ✓Retained testes have approximately 10x higher neoplastic risk than scrotal testes; Sertoli cell tumors and seminomas are the most clinically significant neoplasms.
- ✓Sertoli cell tumor hyperestrogenism can cause alopecia, gynecomastia, and life-threatening bone marrow suppression — screen with CBC before surgery.
- ✓All cryptorchid dogs should undergo complete bilateral orchidectomy at 6 months and must not be used for breeding due to heritable genetics.
- ✓Abdominal orchidectomy requires midline celiotomy; trace the ductus deferens from the prostate or gonadal vessels from major vessels to locate the testicle.
- ✓Post-operative CBC monitoring is essential in Sertoli cell tumor cases to confirm bone marrow recovery from estrogen suppression within 1–3 months.
Classification, Inheritance, and Diagnosis
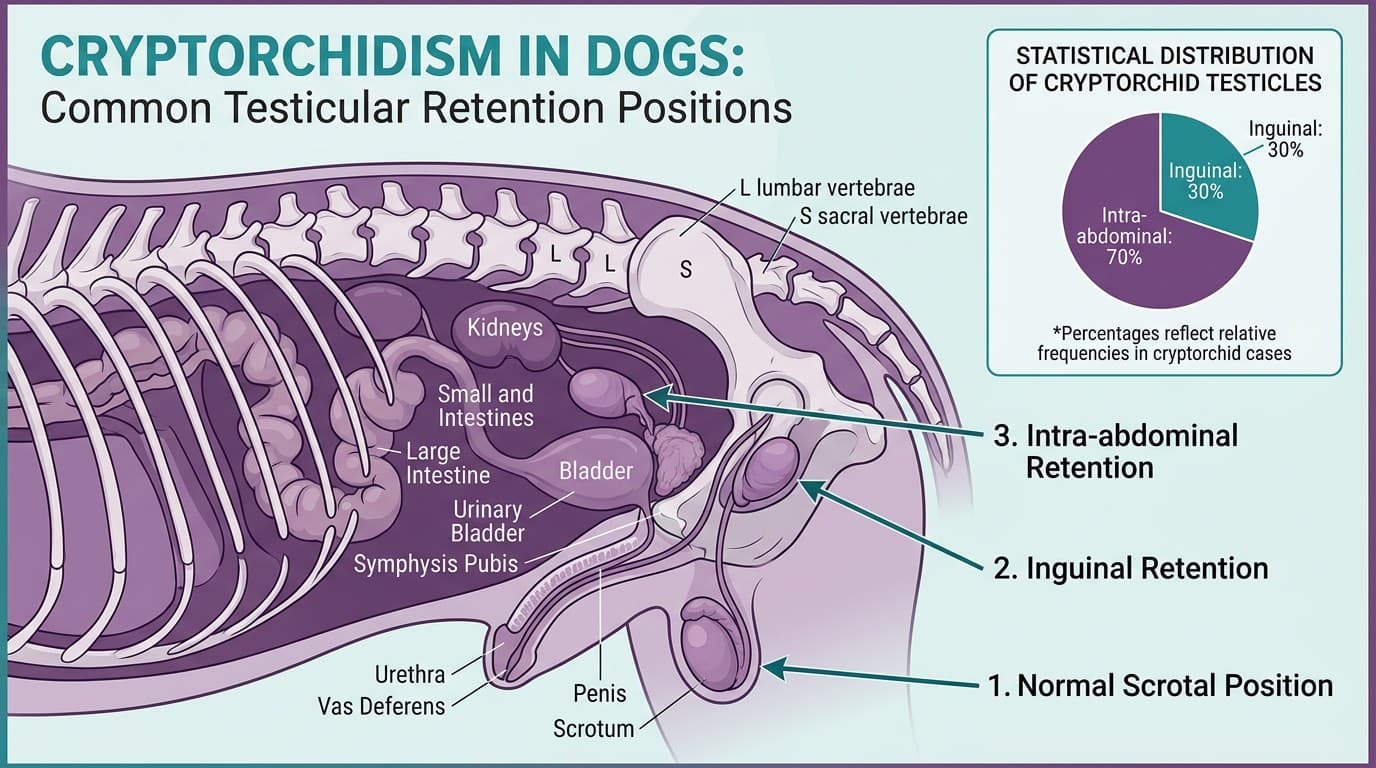
Cryptorchidism is failure of one or both testes to complete their descent from the abdominal cavity through the inguinal canal into the scrotum. Normal descent is complete by 6–8 weeks of age in dogs; a testicle absent from the scrotum at 4–6 months should be considered cryptorchid.
Classification
| Type | Definition | Frequency |
|---|---|---|
| Unilateral | One testicle retained, one in scrotum | ~75% of cryptorchid dogs |
| Bilateral | Both testicles retained | ~25% |
| Right-sided retention | Right testicle retained | More common than left |
| Inguinal retention | Testicle palpable in inguinal region | ~30% of retained testes |
| Abdominal retention | Testicle not palpable externally | ~70% of retained testes |
Genetics Cryptorchidism is inherited as a polygenic or sex-limited autosomal recessive trait in most breeds. Breeds with highest prevalence include: miniature Schnauzer, Pomeranian, Shetland Sheepdog, Chihuahua, Yorkshire Terrier, Boxer, Pekingese, English Bulldog, and Maltese.
Cryptorchid dogs should NOT be used for breeding even if the retained testicle is later descended or surgically retrieved.
Diagnosis
| Method | Finding |
|---|---|
| Physical examination | Absent testicle in scrotum; possible inguinal mass |
| Abdominal palpation | Large retained testicle may be palpable in caudal abdomen |
| Abdominal ultrasound | Identifies testicle location; characterizes tissue; screens for neoplastic changes |
| hCG stimulation test | Confirms presence of testicular tissue if bilateral cryptorchidism vs true absence (anorchidism) |
Ultrasound is recommended for all suspected abdominal cryptorchid cases to plan surgical approach and screen for concurrent neoplasia.
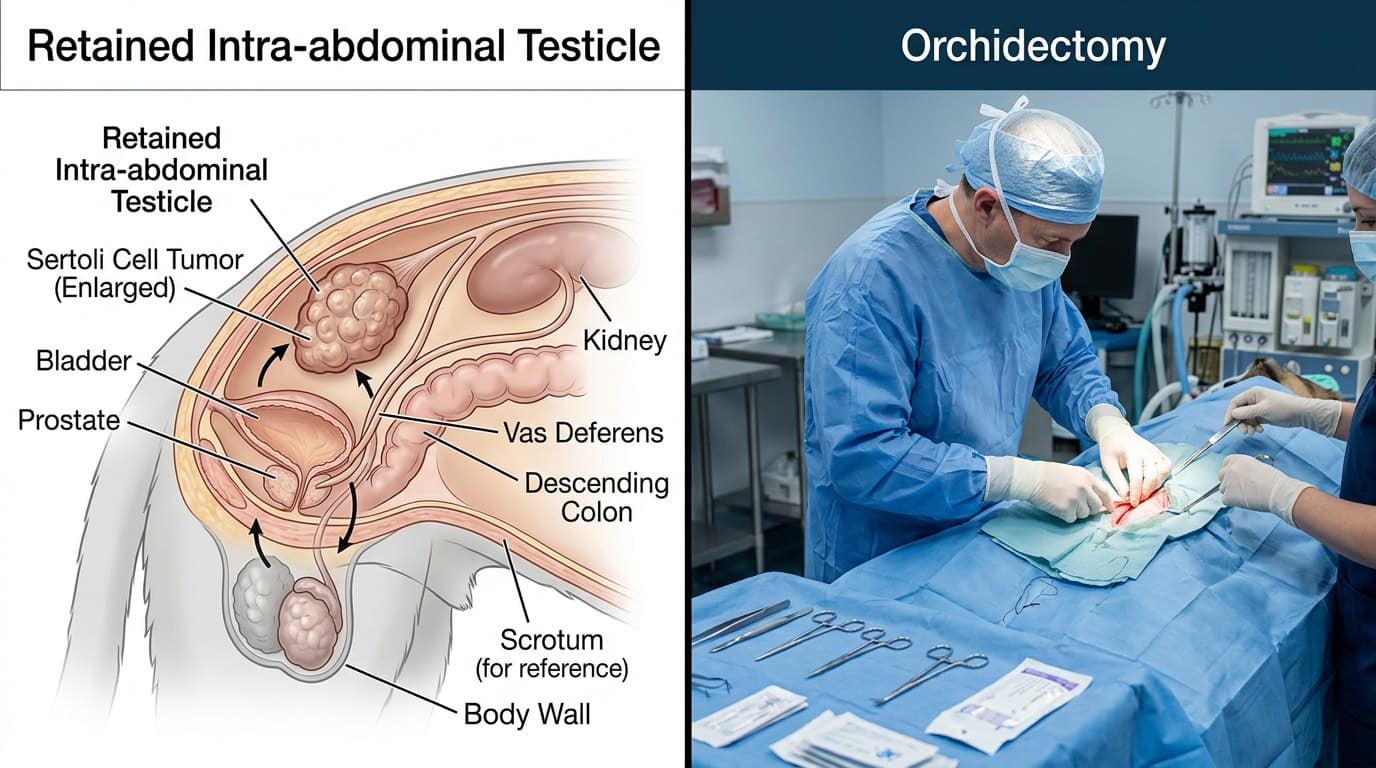
Neoplasia Risk in Retained Testes: Sertoli Cell Tumor and Seminoma
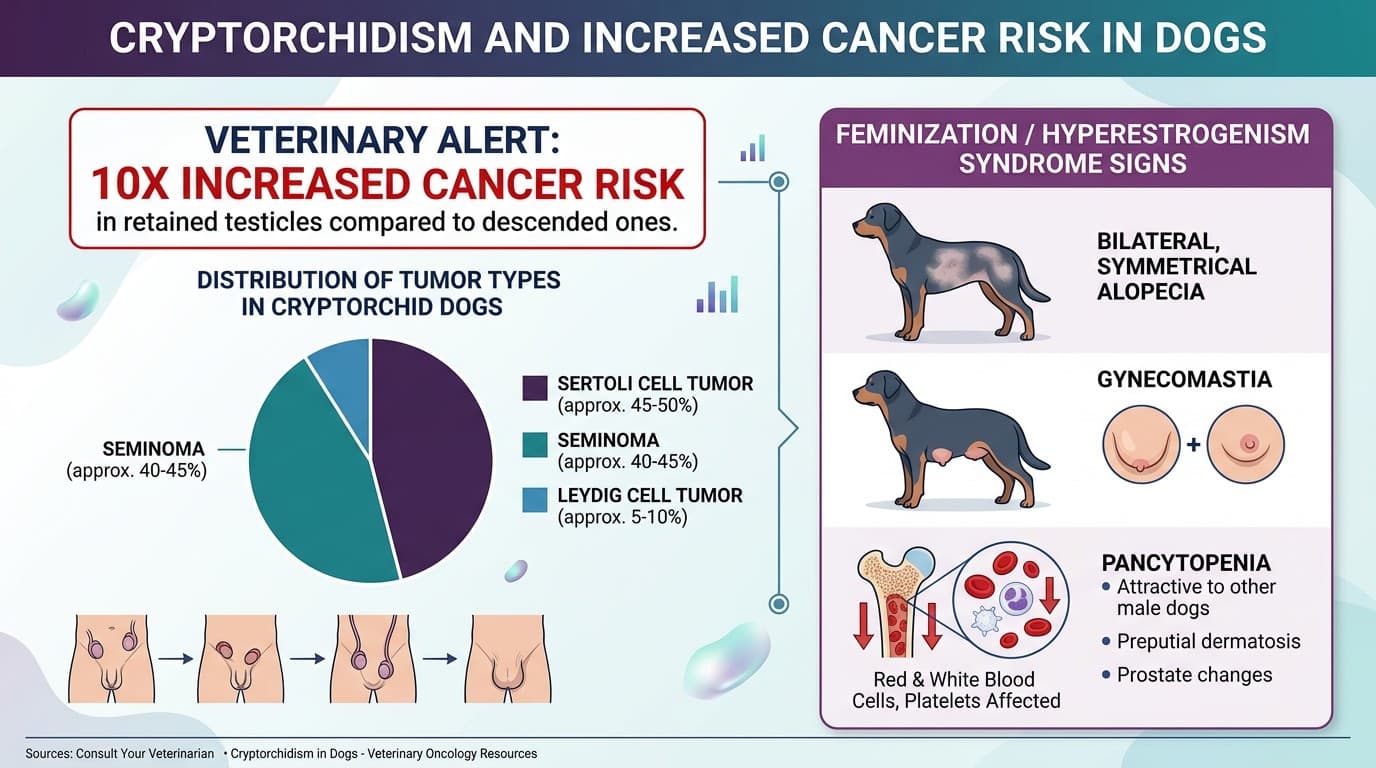
Retained testes are exposed to higher core body temperature (37–38°C vs normal scrotal temperature of 31–33°C), which impairs spermatogenesis and dramatically increases neoplastic transformation risk. Dogs with retained testes are approximately 10 times more likely to develop testicular neoplasia than dogs with normally descended testes.
Tumor Types Associated with Cryptorchid Testes
| Tumor | Characteristics | Notes |
|---|---|---|
| Sertoli cell tumor | Most common in cryptorchid testes; may produce estrogen | Hyperestrogenism syndrome in 25–50% |
| Seminoma | Common in abdominal testicles; locally invasive | Metastatic rate ~5–10% |
| Interstitial (Leydig) cell tumor | Less common in cryptorchid; more common in scrotal testes | Rarely malignant |
Hyperestrogenism Syndrome from Sertoli Cell Tumor
- Bilateral symmetrical alopecia
- Gynecomastia (mammary gland enlargement)
- Pendulous prepuce, small contralateral testicle
- Bone marrow suppression (pancytopenia) — potentially fatal
- Perineal adenocarcinoma-like skin changes
Management of Sertoli Cell Tumor with Bone Marrow Suppression
- CBC before surgery: if severe thrombocytopenia (<50,000/uL) or neutropenia, delay surgery until marrow partially recovers
- Blood transfusion may be required pre-operatively
- Bone marrow suppression typically reverses within 1–3 months post-orchidectomy
Metastatic Potential
| Tumor | Metastatic Rate |
|---|---|
| Sertoli cell tumor | 10–15% |
| Seminoma | 5–10% |
| Interstitial cell tumor | <1% |
Abdominal radiographs and lymph node assessment (iliac lymph nodes) recommended for Sertoli cell and seminoma cases before surgery.
Orchidectomy Approach: Inguinal vs Paramedian vs Flank Incision
All cryptorchid dogs should undergo orchidectomy regardless of age — retained testes carry substantial cancer risk and all cryptorchid dogs should be desexed to prevent passage of the trait to offspring. Timing: recommended at 6 months unless clinical signs of neoplasia require earlier intervention.
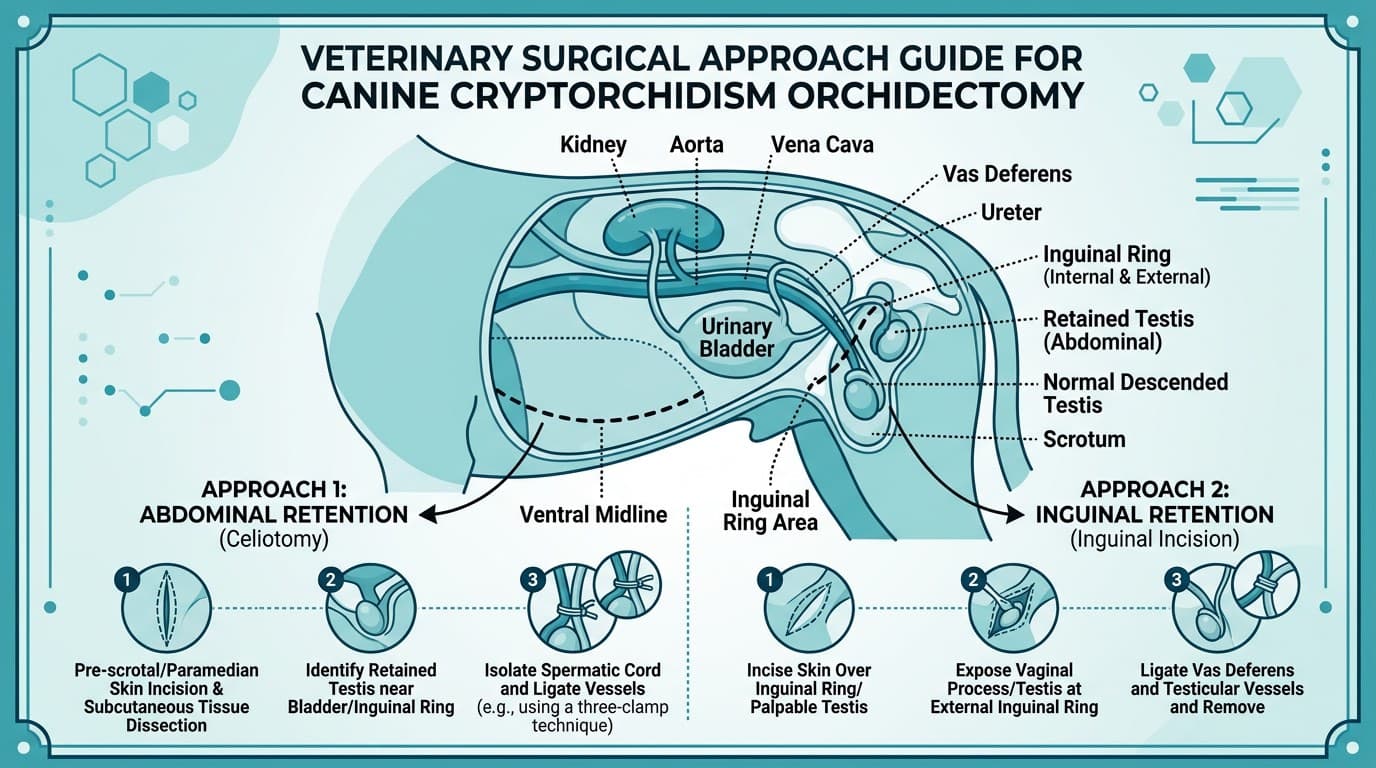
Surgical Approach Selection
| Retention Location | Recommended Approach |
|---|---|
| Inguinal (palpable) | Inguinal incision directly over the testicle |
| Pre-scrotal inguinal | Modified inguinal approach or mid-line |
| Abdominal — small testicle | Paramedian or midline celiotomy |
| Abdominal — suspected neoplasia | Midline celiotomy; wide exposure for lymph node assessment |
| Bilateral cryptorchidism | Both testicles via same or staged approach |
Inguinal Orchidectomy
- Incision over external inguinal ring
- Identify the gubernaculum or testicular cord
- Ligate spermatic cord (artery + vein) separately or en masse
- Do NOT leave inguinal fat pad attached to spermatic cord — it can retract into the canal
Abdominal Orchidectomy (Midline Celiotomy)
- Enter abdomen via midline incision caudal to umbilicus
- Identify testicle: typically lateral to the bladder, associated with the ductus deferens
- Trace the ductus deferens cranially to locate the gonadal vessels
- Double ligate the spermatic artery and vein before transection
- Palpate and visually inspect iliac lymph nodes for enlargement
Post-Operative Care
- Standard castration recovery
- If concurrent Sertoli cell tumor: recheck CBC at 4–6 weeks, then monthly until bone marrow recovery confirmed
- Repeat abdominal ultrasound at 4 weeks if neoplasia was confirmed to screen for local recurrence
Frequently Asked Questions
At what age should a cryptorchid dog be neutered?
Orchidectomy is recommended at 6 months for cryptorchid dogs. If signs of testicular neoplasia are present (feminization, abdominal mass), surgery should be performed immediately regardless of age.
Can a cryptorchid testicle descend on its own after 6 months?
Spontaneous descent after 6 months is extremely rare. A testicle absent from the scrotum at 4–6 months should be considered permanently retained, and orchidectomy should be planned.
Will the scrotal testicle in a unilateral cryptorchid dog be fertile?
The scrotal testicle is fertile, but cryptorchid dogs should not be bred because the trait is heritable. All cryptorchid dogs should undergo complete orchidectomy (both testes removed) regardless of whether only one testicle is retained.
What are the signs of a Sertoli cell tumor in a dog?
Classic signs include bilateral symmetrical flank alopecia, gynecomastia (enlarged mammary glands), small contralateral testicle, pendulous prepuce, and possible bone marrow suppression causing bruising or infection susceptibility. An abdominal mass may be palpable.
How do you find a retained abdominal testicle during surgery?
Locate the ductus deferens at the prostate and trace it cranially — it will lead directly to the retained testicle. Alternatively, trace the gonadal vessels from the aorta (left) or caudal vena cava (right) caudally. Ultrasound-guided marking pre-operatively is helpful for very small testes.
References
- Hayes HM, Pendergrass TW. Canine testicular tumors: epidemiologic features of 410 dogs. Int J Cancer. 1976;18(4):482-487.
- Reif JS, Maguire TG, Kenney RM, Brodey RS. A cohort study of canine testicular neoplasia. J Am Vet Med Assoc. 1979;175(7):719-723.
- Pendergrass TW, Hayes HM Jr. Cryptorchidism and related defects in dogs: epidemiologic comparisons with man. Teratology. 1975;12(1):51-55.