
Quick Answer
Pain is the most common presenting complaint in veterinary medicine yet remains the most undertreated. This guide covers species-specific behavioral indicators, validated acute and chronic pain scales, intervention thresholds, and multimodal analgesia principles.
Key Takeaways
- ✓Pain is the most undertreated condition in veterinary medicine — use validated scales to objectify assessment and justify intervention
- ✓Glasgow CMPS-SF: maximum 24, intervene at ≥5–6. UNESP-Botucatu cats: maximum 30, intervene at ≥7. FGS: intervene at ≥4/10
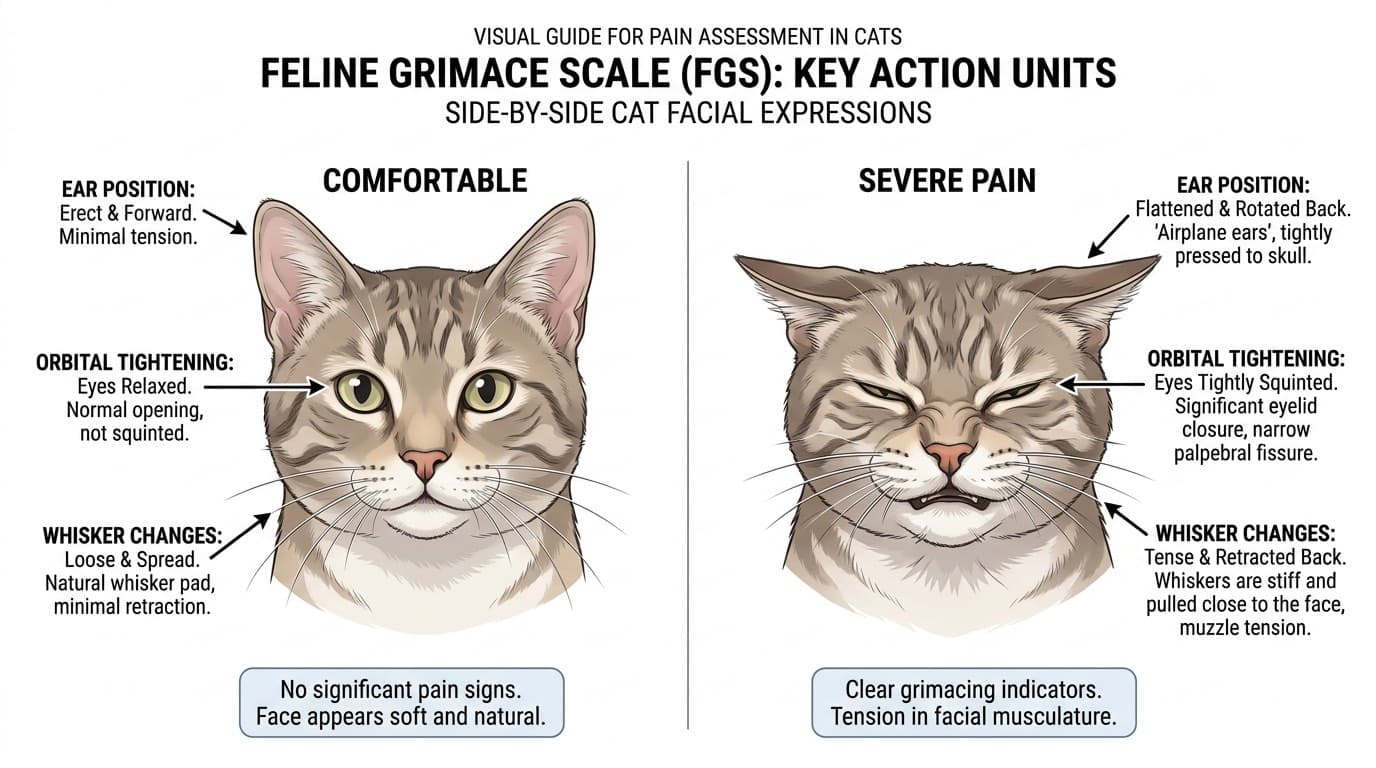
- ✓Cats mask pain especially well in unfamiliar environments — always use the Feline Grimace Scale, not subjective impression
- ✓Multimodal analgesia targets multiple pain pathway points simultaneously, achieving superior control at lower doses of each drug
- ✓Local anesthetic nerve blocks provide excellent analgesia with no systemic side effects — underutilized in general practice
- ✓Gabapentin 5–10 mg/kg BID–TID is the primary analgesic for neuropathic and chronic pain in both dogs and cats
Why Objective Pain Assessment Matters
Pain is both a clinical sign and a welfare concern. Untreated or undertreated pain in veterinary patients leads to:
- Physiological consequences: Increased sympathetic tone, elevated cortisol, immunosuppression, delayed wound healing, ileus, urinary retention, cardiovascular stress
- Behavioral consequences: Aggression, fear responses, reduced appetite, sleep disruption
- Wind-up and central sensitization: Inadequately treated acute pain can progress to chronic pain states (central sensitization) that are significantly harder to treat
The challenge of veterinary pain assessment: Patients cannot self-report pain verbally. Reliance on subjective "gut feel" leads to significant inter-observer variability and systematic undertreatment — especially in stoic species (cats), prey animals, and animals that inhibit pain displays in unfamiliar environments.
Validated pain scales solve this problem: By providing structured behavioral observation criteria with numerical scores, validated scales reduce inter-observer variability, create a documentation trail, identify intervention thresholds, and allow tracking of treatment response over time.
Behavioral Indicators of Pain by Species
Canine Pain Behaviors
- Vocalization: whimpering, yelping, groaning — especially on handling
- Altered posture: hunched, guarded, "prayer position" (elbow-down, hindquarters elevated — indicates abdominal pain)
- Facial expression: furrowed brow, orbital tightening, raised inner brow (Canine Facial Action Coding System)
- Reduced activity: reluctance to move, rest, or change positions
- Agitation/restlessness: pacing, inability to settle (especially with visceral pain)
- Reduced interaction and appetite
- Protecting/guarding injured area
Feline Pain Behaviors — Subtler and Easily Missed
- Feline Grimace Scale (FGS) indicators: orbital tightening (squinted eyes), muzzle tension, whisker change (bunched forward), ear position (flattened/rotated), head position (down/below shoulder line)
- Reduced activity, hiding, hunched posture
- Decreased grooming OR excessive grooming/licking of painful area
- Reduced appetite, decreased interaction
- Tail flicking, flattened ears (immediate response to touch)
- Changes in facial expression (easier to detect in chronic pain than acute)
Species-specific caution: Cats routinely hide pain to avoid appearing vulnerable. A cat sitting quietly in a cage should NOT be assumed to be comfortable — always assess systematically using a validated scale.
Validated Pain Scales: Glasgow, Colorado State, UNESP-Botucatu
Glasgow Composite Measure Pain Scale — Short Form (CMPS-SF) for Dogs The most widely validated acute pain scale for dogs. 30 behavioral descriptors across 6 categories: 1. Vocalization 2. Attention to wound 3. Mobility 4. Response to touch 5. Demeanor 6. Body tension/posture
Maximum score: 24. Intervention threshold: ≥5/24 (or ≥6/24 for surgeries). Scores above this threshold indicate pain requiring analgesia.
Available free online from the University of Glasgow.
Colorado State University Pain Scale (dogs and cats)
- Score 2: Uncomfortable when area palpated; analgesic indicated
- Score 3–4: Consistently uncomfortable; analgesic required
UNESP-Botucatu Multidimensional Composite Pain Scale for Cats
- Pain expression (facial expression, body posture, comfort)
- Psychomotor change
- Physiological variables (blood pressure)
Maximum score: 30. Intervention at ≥7/30.
Feline Grimace Scale (FGS) Validated for acute pain in cats. Five Action Units scored 0–2 each (maximum 10). Intervention threshold: ≥4/10. Free download: www.felinegrimacescale.com
Multimodal Analgesia: Principles and Drug Classes
Multimodal analgesia uses drugs from different classes to target multiple points in the pain pathway simultaneously. This achieves superior pain control at lower doses of each individual drug, reducing side effects.
The Pain Pathway Targets: 1. Peripheral sensitization (inflammation): NSAIDs, steroids 2. Nociceptor activation: Local anesthetics (blocks transmission) 3. Spinal cord transmission (dorsal horn): NMDA antagonists (ketamine), alpha-2 agonists 4. Central perception: Opioids, gabapentin/pregabalin
Drug Classes and Clinical Use:
NSAIDs (COX inhibitors): Meloxicam, carprofen, robenacoxib, grapiprant (LGIT agonist). First-line analgesics for most acute and chronic pain. Avoid in hypovolemic, renal-compromised, or GI-compromised patients.
Opioids: Morphine, hydromorphone, buprenorphine, fentanyl, methadone. Excellent perioperative analgesia. Buprenorphine (buccal 0.01–0.03 mg/kg q6–8h) is the most practical opioid for cats.
Local Anesthetics: Lidocaine, bupivacaine, ropivacaine. Nerve blocks (locoregional), epidurals, line blocks, wound soaker catheters. Highly effective with no systemic side effects when used correctly.
Ketamine (NMDA antagonist): Sub-anesthetic doses (0.1–0.6 mg/kg/hr CRI) prevent wind-up and central sensitization. Invaluable in CRI protocols for major surgeries.
Gabapentin/Pregabalin: Alpha-2-delta calcium channel modulators. Primary use in neuropathic and chronic pain. Dose: gabapentin 5–10 mg/kg BID–TID in dogs; 5–10 mg/kg BID in cats.
Alpha-2 agonists (dexmedetomidine): Excellent short-term sedation and analgesia (CRI or intermittent dosing). Avoid in cardiovascular disease.
Example perioperative multimodal protocol (orthopedic surgery): Pre-op: NSAID + opioid premedication Intraoperative: locoregional nerve block + ketamine CRI Post-op: NSAID q24h + gabapentin BID + tramadol PRN for breakthrough pain
References
- Morton CM, et al. Application of a scaling model to establish and validate an interval level pain scale for assessment of acute pain in dogs. Am J Vet Res. 2005.
- Steagall PV, Monteiro BP. Acute pain in cats: recent advances in clinical assessment. J Feline Med Surg. 2019.
- Mathews K, et al. WSAVA Guidelines for recognition, assessment and treatment of pain. J Small Anim Pract. 2014.