
Quick Answer
A comprehensive guide to feline infectious peritonitis covering feline coronavirus mutation, the distinction between effusive and non-effusive forms, diagnostic challenges, the revolutionary GS-441524 antiviral treatment, and current prognosis.
Key Takeaways
- ✓FIP develops when common feline enteric coronavirus mutates within an individual cat — it is not directly contagious as FIP from cat to cat.
- ✓FIP presents in wet (effusive) and dry (non-effusive) forms, with wet FIP being more common and easier to diagnose.
- ✓GS-441524 antiviral treatment has transformed FIP from a universally fatal disease to one with 80–90% remission rates.
- ✓Treatment requires a minimum 84-day course of daily antiviral medication, with higher doses needed for neurological and ocular forms.
- ✓Cats achieving sustained remission 3 months post-treatment are generally considered cured with normal life expectancy.
Understanding FIP
Feline infectious peritonitis (FIP) has long been considered one of the most devastating and feared diagnoses in feline medicine. It is caused by a mutated form of feline coronavirus (FCoV), a ubiquitous virus that is extremely common in cat populations worldwide — particularly in multi-cat environments such as catteries, shelters, and multi-cat households, where infection rates can approach 80 to 90 percent.
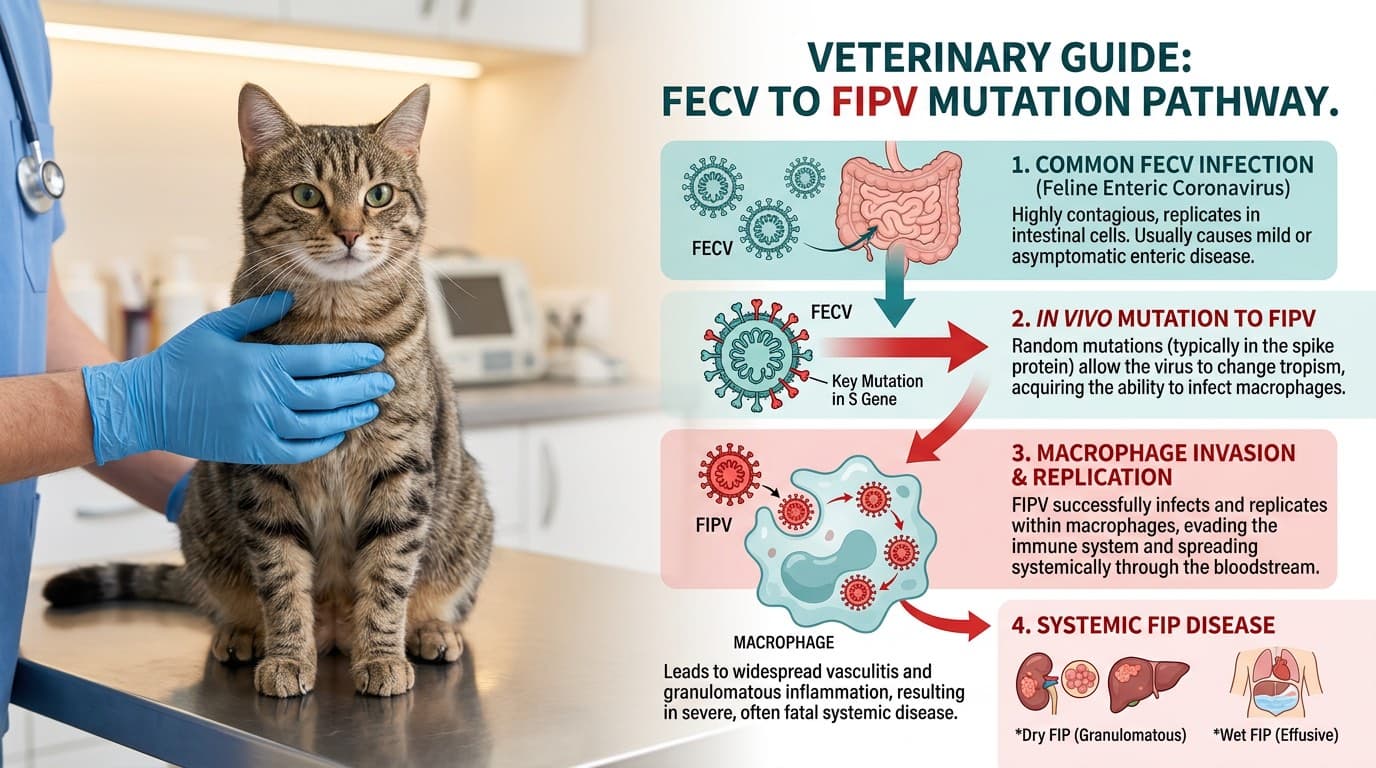
The critical distinction is between feline enteric coronavirus (FECV), which is the harmless intestinal form that most cats carry without consequence, and the virulent biotype known as feline infectious peritonitis virus (FIPV), which arises from spontaneous mutations within an individual cat's own enteric coronavirus population. These mutations enable the virus to infect and replicate within macrophages (a type of white blood cell), triggering a systemic and often fatal immune-mediated vasculitis and granulomatous inflammatory disease.
Importantly, FIP itself is not directly contagious from cat to cat. What spreads between cats is the common enteric coronavirus, and the mutation to the virulent FIP-causing form occurs independently within individual cats. Most cats that carry feline enteric coronavirus never develop FIP — the mutation and subsequent disease develops in an estimated 5 to 12 percent of infected cats, typically those with immature or compromised immune systems.
Until recently, FIP was considered universally fatal. However, the development of antiviral drugs — particularly GS-441524 (a nucleoside analogue closely related to remdesivir) — has fundamentally transformed the prognosis and created a new era in FIP treatment, with cure rates exceeding 80 percent in treated cats.
Wet vs Dry FIP
FIP manifests in two classical forms, though many cats present with features of both. The form that develops is believed to depend on the balance between the cat's cell-mediated and humoral immune responses.
Effusive (Wet) FIP
The effusive form is the more common and more rapidly progressive presentation. It is characterized by the accumulation of a distinctive protein-rich, straw-colored to golden-yellow fluid in the abdominal cavity (ascites), thoracic cavity (pleural effusion), or pericardial sac. The fluid has a characteristically high protein content (usually greater than 3.5 g/dL), low cellularity, and a viscous, sticky quality.
Clinical signs of wet FIP include:
- Progressive abdominal distension (fluid belly)
- Difficulty breathing if pleural effusion is present
- Persistent fluctuating fever that does not respond to antibiotics
- Weight loss and progressive lethargy
- Decreased appetite
- Jaundice (yellow discoloration of the gums and skin)
Wet FIP typically progresses rapidly — often over days to weeks — and historically carried a median survival of just 9 days from diagnosis without treatment.
Non-effusive (Dry) FIP
The dry form develops when the cat mounts a partial cell-mediated immune response that limits fluid accumulation but allows granulomatous (nodular) inflammation to develop in various organs. The clinical presentation depends entirely on which organs are affected:
- Eyes — uveitis (inflammation of the uveal tract), keratic precipitates ("mutton fat" deposits on the cornea), color change of the iris, and retinal changes
- Central nervous system — ataxia, seizures, behavioral changes, head tilt, nystagmus, hindlimb paresis
- Kidneys — irregular, enlarged kidneys with granulomatous nodules
- Liver — hepatomegaly, icterus, elevated liver enzymes
- Intestines — thickened intestinal walls, mesenteric lymphadenopathy
Dry FIP is more diagnostically challenging because it can mimic many other diseases and lacks the dramatic effusions that make wet FIP more immediately recognizable. Neurological and ocular FIP can be particularly difficult to diagnose definitively without advanced testing.

Diagnostic Challenges
Diagnosing FIP remains one of the most challenging tasks in feline medicine because no single non-invasive test is definitively diagnostic on its own. Diagnosis requires synthesizing clinical signs, laboratory findings, imaging, and effusion analysis.
Effusion Analysis (Wet FIP)
When effusion is present, fluid analysis provides the strongest diagnostic evidence:
- High protein — total protein greater than 3.5 g/dL with an albumin:globulin ratio below 0.4 is highly suggestive
- Rivalta test — a simple point-of-care test where a drop of effusion is placed in acetic acid; a positive result (the drop retains its shape and floats) has high sensitivity for FIP
- Immunocytochemistry — staining macrophages in the effusion for FCoV antigen is highly specific but not always available
- RT-PCR — detection of feline coronavirus RNA in effusion fluid by PCR supports the diagnosis
Blood Tests
Routine bloodwork often shows:
- Hyperglobulinemia (elevated globulins, particularly gamma-globulins)
- Low albumin:globulin ratio (below 0.6 is suspicious, below 0.4 is highly suggestive)
- Non-regenerative anemia
- Elevated bilirubin (jaundice)
- Lymphopenia (decreased lymphocyte count)
Coronavirus Antibody Titers
FCoV antibody testing is widely available but has significant limitations. A positive antibody titer simply confirms exposure to feline coronavirus — which is nearly universal in multi-cat environments — and does not distinguish harmless enteric infection from FIP. A negative titer makes FIP less likely but does not rule it out, as some FIP cats have low or undetectable titers (particularly in end-stage disease).
Advanced Diagnostics
Immunohistochemistry on tissue biopsies (identifying FCoV antigen within macrophages in affected tissues) remains the gold standard for definitive diagnosis. However, obtaining biopsies from critically ill cats carries significant anesthetic and surgical risk. In practice, most clinicians make a presumptive diagnosis based on the combination of compatible clinical signs, supportive laboratory findings, and effusion characteristics, and then confirm the diagnosis indirectly through treatment response.

GS-441524 & Antiviral Treatment
The development of effective antiviral therapy for FIP represents one of the most significant breakthroughs in feline medicine in decades. What was once a uniformly fatal diagnosis now has cure rates exceeding 80 percent with appropriate treatment.
GS-441524 — The Game-Changer
GS-441524 is a nucleoside analogue that inhibits viral RNA-dependent RNA polymerase, effectively stopping coronavirus replication. It is the active metabolite of remdesivir (the human antiviral used during the COVID-19 pandemic). Research pioneered by Dr. Niels Pedersen at UC Davis demonstrated dramatic efficacy in naturally occurring FIP cases, with the majority of cats achieving sustained remission.
Treatment Protocol
The standard GS-441524 treatment protocol involves:
- Route — subcutaneous injection daily (the most extensively studied route) or oral administration (increasingly available and effective)
- Dose — typically 4–8 mg/kg for non-neurological/non-ocular FIP, with higher doses (8–12 mg/kg) recommended for neurological and ocular forms because the drug must cross the blood-brain/blood-ocular barriers
- Duration — minimum 84 days (12 weeks) of continuous daily treatment
- Monitoring — regular rechecks including physical examination, bloodwork (globulins, albumin:globulin ratio, hematocrit), and clinical assessment
Most cats show dramatic clinical improvement within the first 3 to 5 days of treatment — fever resolves, appetite returns, energy levels increase, and effusions begin to resolve. This rapid response serves as additional diagnostic confirmation.
Molnupiravir — An Alternative
Molnupiravir, another antiviral originally developed for human use, has also shown efficacy against FIP. It works by a different mechanism (mutagenesis of the viral genome) and is available in oral form. Some practitioners use it as first-line therapy or as a rescue agent for cases that relapse after GS-441524 treatment.
Regulatory Status
As of early 2026, GS-441524 has received conditional approval from the USDA for veterinary use in treating FIP in cats, making it legally available through licensed veterinarians. This followed years during which the drug was only available through gray-market sources, creating significant ethical and legal challenges for the veterinary profession. The availability of regulated, quality-controlled formulations has been a major step forward for both efficacy and safety.
Cost Considerations
Treatment cost varies by the cat's weight, the required dose, and the formulation used, but a full 84-day course typically ranges from $2,000 to $6,000 or more. While substantial, this represents a life-saving treatment for a previously fatal disease, and many owners find it a worthwhile investment.

Prognosis & Prevention
Prognosis with Treatment
The prognosis for FIP has been transformed by antiviral therapy. Published studies report remission rates of 80 to 90 percent for cats completing a full 84-day treatment course with GS-441524. Cats with effusive (wet) FIP generally respond faster and more predictably than those with non-effusive (dry) forms, though both are treatable. Neurological FIP historically carried the lowest response rates, but higher-dose protocols have significantly improved outcomes even for these challenging cases.
Relapse can occur in approximately 10 to 15 percent of treated cats, usually within the first few months after completing treatment. Relapsed cases are typically re-treated with a higher dose or an alternative antiviral (molnupiravir), and many achieve sustained remission on the second course.
Cats that complete treatment and remain in remission for 3 months after finishing therapy are generally considered cured and can be expected to live normal lifespans.
Prevention Strategies
Because feline enteric coronavirus is the precursor to FIP and is nearly impossible to eliminate from multi-cat environments, prevention focuses on reducing viral load and supporting immune function:
- Stress reduction — stress is a major factor in FIP development; minimizing overcrowding, maintaining stable social groups, and providing adequate resources (litter boxes, food stations, resting areas) reduce risk
- Litter box hygiene — feline coronavirus is shed primarily in feces. Scooping litter boxes at least daily, using separate boxes for kittens, and periodic disinfection with dilute bleach reduce fecal-oral transmission
- Early weaning in high-risk catteries — isolating kittens at 5–6 weeks of age from coronavirus-shedding adults can reduce early infection, though this approach requires careful management to avoid behavioral issues
- Immune support — ensuring kittens receive adequate colostrum, maintaining good nutrition, and minimizing unnecessary stressors support immune competence during the vulnerable period
An intranasal FIP vaccine (Primucell FIP) exists but has limited efficacy and is not routinely recommended by most veterinary immunologists. The most practical prevention remains reducing coronavirus exposure and minimizing stress in multi-cat environments.

Frequently Asked Questions
Is FIP contagious to other cats in my household?
FIP itself is not directly contagious between cats. What spreads is the common feline enteric coronavirus, which most cats carry harmlessly. The mutation to FIP-causing virus occurs independently within individual cats. Other cats in the household may carry coronavirus but are not at significantly elevated risk of developing FIP solely from living with an affected cat.
How much does FIP treatment cost?
A full 84-day treatment course with GS-441524 typically costs $2,000 to $6,000 depending on the cat's weight, the required dosage, and the specific formulation used. Neurological and ocular FIP require higher doses and may cost more. Additional expenses include diagnostic workup and regular monitoring bloodwork during treatment.
Can FIP be cured completely?
Yes. With the advent of GS-441524 and other antiviral therapies, FIP can now be cured in the majority of cases. Studies show remission rates of 80–90% for cats completing the full treatment course. Cats that remain in remission for 3 months after finishing treatment are generally considered cured and live normal lifespans.
How is FIP diagnosed?
FIP diagnosis combines clinical signs, bloodwork (low albumin:globulin ratio, hyperglobulinemia), imaging, and effusion analysis when fluid is present. The Rivalta test and PCR on effusion fluid are particularly useful for wet FIP. No single blood test is definitive — diagnosis is based on the overall clinical picture. Response to antiviral treatment provides retrospective confirmation.
At what age are cats most susceptible to FIP?
FIP most commonly affects young cats between 3 months and 2 years of age, when the immune system is still maturing. A second, smaller peak occurs in cats over 10 years old, potentially due to age-related immune decline. Purebred cats and cats from multi-cat environments (shelters, catteries) are at higher risk.
References
- Pedersen NC, et al. Efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. Journal of Feline Medicine and Surgery. 2019;21(4):271-281.
- Addie DD, et al. Oral mutian GS-441524 antiviral treatment for cats with clinically diagnosed neurological feline infectious peritonitis. Journal of Feline Medicine and Surgery. 2020;22(12):1165-1174.
- Tasker S. Diagnosis of feline infectious peritonitis: update on evidence supporting available tests. Journal of Feline Medicine and Surgery. 2018;20(3):228-243.
- Murphy BG, et al. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Veterinary Microbiology. 2018;219:141-149.