
Quick Answer
Congestive heart failure (CHF) is one of the most common serious conditions in middle-aged and senior dogs. This comprehensive guide covers the underlying causes, early warning signs, how veterinarians diagnose CHF, evidence-based treatment options, and how to help your dog live comfortably with this manageable condition.
Key Takeaways
- ✓CHF is the end-stage of cardiac disease where fluid accumulates in lungs or abdomen; the most common cause in dogs is myxomatous mitral valve disease (MMVD)
- ✓Cavalier King Charles Spaniels, Dachshunds, and Dobermans are at highest risk and should be screened regularly
- ✓Increased resting respiratory rate (>30 breaths/min sleeping) is the earliest and most sensitive sign of pulmonary edema — monitor this daily at home
- ✓The ACVIM 2019 guidelines recommend starting pimobendan in Stage B2 (pre-CHF) dogs with enlarged hearts to delay onset of failure by ~15 months
- ✓Stage C CHF is treated with the triple-drug protocol: furosemide + pimobendan + ACE inhibitor
- ✓Sodium-restricted diet, omega-3 supplementation, gentle exercise, and stress reduction are important supportive measures
- ✓With good management, many dogs live 1–2 years after CHF diagnosis with good quality of life
What Is Congestive Heart Failure?
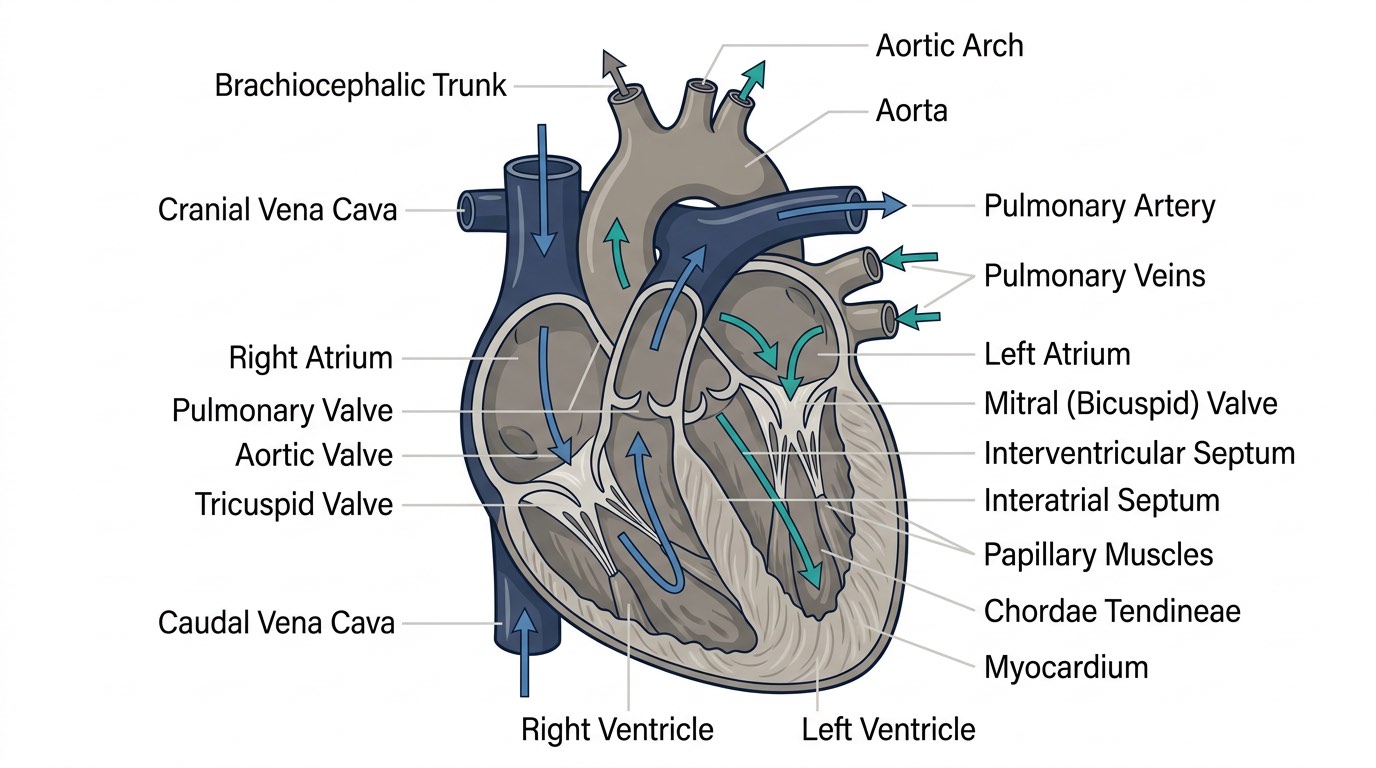
Congestive heart failure (CHF) is not a disease in itself but a syndrome — the endpoint of various cardiac conditions that leave the heart unable to pump blood efficiently enough to meet the body's needs. When the heart fails to maintain adequate cardiac output, fluid accumulates ("congests") in the lungs, chest cavity, or abdomen, depending on which side of the heart is primarily affected.
In dogs, CHF is divided by affected side:
- Left-sided CHF: The left ventricle fails to pump blood forward into the systemic circulation. Blood backs up into the pulmonary vasculature, causing fluid to leak into the lung tissue (pulmonary edema) or pleural space. This is by far the most common form in dogs and causes the hallmark cough and labored breathing owners notice first.
- Right-sided CHF: The right ventricle fails to pump blood into the pulmonary circulation. Blood backs up into the systemic venous system, causing fluid accumulation in the abdomen (ascites), pleural effusion, and limb edema. Right-sided CHF is less common in isolation but can occur with pulmonary hypertension, pericardial disease, or tricuspid valve disease.
- Biventricular CHF: Both sides fail simultaneously, typically in advanced or end-stage disease.
CHF is extremely common in dogs — estimates suggest it affects up to 11% of all dogs presenting to general practice. The prevalence rises steeply with age: many breeds have a lifetime risk exceeding 30% by age 10–12 years. Understanding this condition empowers owners to recognize early signs, work proactively with their veterinarian, and help their dog live comfortably for months to years after diagnosis.
Causes and Predisposed Breeds
The two most common underlying cardiac diseases leading to CHF in dogs are:
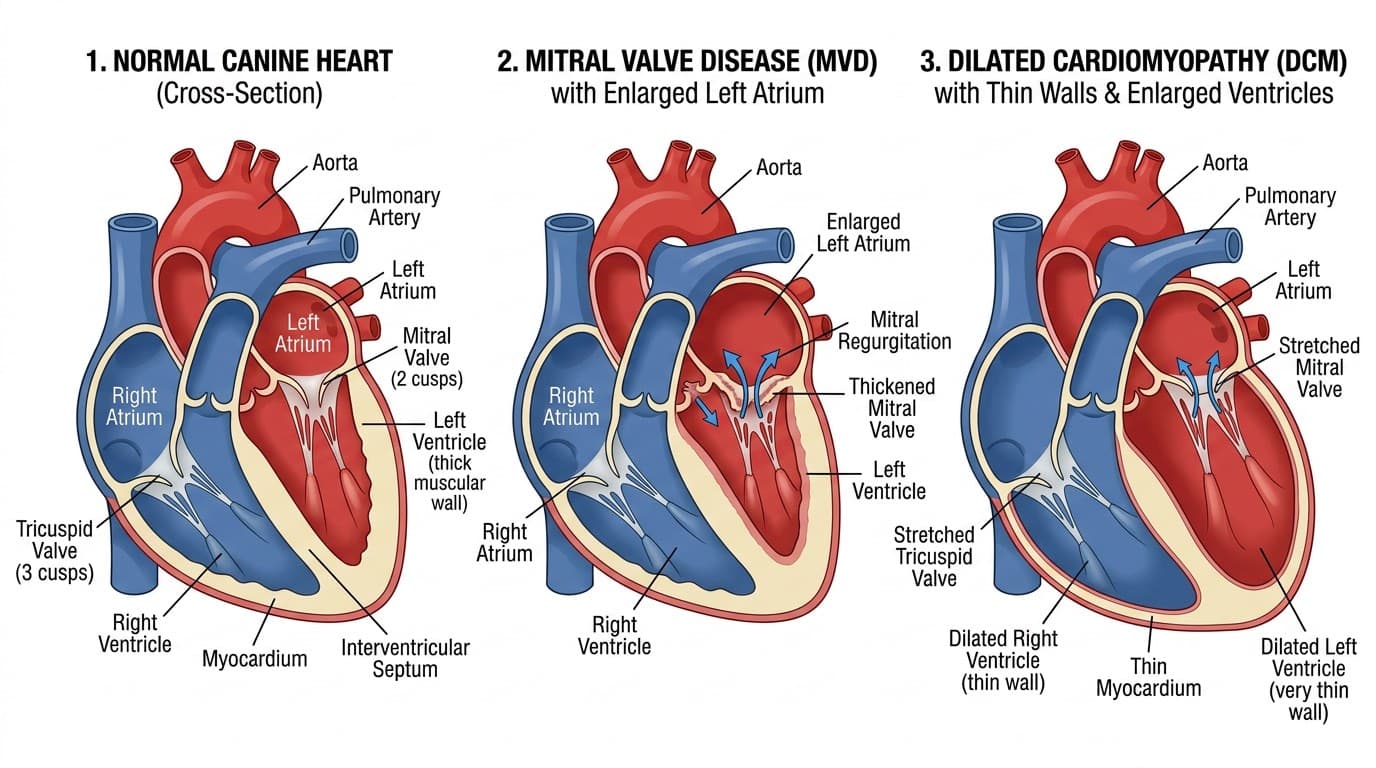
1. Myxomatous Mitral Valve Disease (MMVD)
MMVD — also called chronic valvular disease, degenerative mitral valve disease, or endocardiosis — accounts for approximately 75–80% of all canine cardiac disease. The mitral valve (between the left atrium and ventricle) progressively thickens, nodulates, and deforms, causing regurgitation (backward blood flow) that increases cardiac workload over years. Eventually, the compensatory mechanisms the heart uses to maintain output — dilation, hypertrophy, increased sympathetic tone — are overwhelmed, and CHF develops.
Breeds with significantly elevated MMVD risk include:
- Cavalier King Charles Spaniels: The most affected breed; nearly all develop MMVD by age 10, and many progress to CHF
- Dachshunds, Miniature and Toy Poodles, Chihuahuas, Maltese, Yorkshire Terriers, Schnauzers: All overrepresented
- Small and medium-sized mixed breeds: Also commonly affected
MMVD follows a staging system developed by the American College of Veterinary Internal Medicine (ACVIM, 2019 guidelines), from Stage A (no disease, at-risk breed) through Stage B1 (murmur, no cardiac changes), B2 (murmur with radiographic/echocardiographic remodeling), and Stage C (current or previous CHF) to Stage D (refractory CHF).
2. Dilated Cardiomyopathy (DCM)
DCM is the primary muscle disease of the heart, characterized by dilation and weakened systolic function of the ventricles. It is the second most common cause of CHF in dogs, accounting for roughly 10–15% of cases.
Breeds with high DCM prevalence:
- Doberman Pinschers: The breed most severely affected; occult DCM is present in up to 50% of middle-aged Dobermans before symptoms appear
- Great Danes, Boxers (arrhythmogenic cardiomyopathy), Irish Wolfhounds, Newfoundlands, Scottish Deerhounds, Standard Schnauzers
- Cocker Spaniels: Historically associated with nutritional (taurine-responsive) DCM
DCM can also have nutritional components — grain-free diets and diets high in legumes have been linked to an increased incidence of DCM in breeds not typically predisposed, though the mechanism and causality remain under investigation by the FDA.
Less Common Causes
- Pericardial effusion (cardiac tamponade)
- Congenital heart defects (patent ductus arteriosus, ventricular septal defect, subaortic stenosis)
- Cardiac arrhythmias causing sustained low output
- Heartworm disease (causing right-sided failure)
- Infectious endocarditis
Recognizing the Signs of CHF
CHF develops progressively. In the early compensated phase (Stage B), dogs are often completely asymptomatic despite significant cardiac changes — which is why regular veterinary auscultation matters for at-risk breeds. Once compensation fails, clinical signs emerge, and prompt recognition is critical.
Early Warning Signs (often subtle)
- Increased resting respiratory rate (RRR) — *the most sensitive early indicator of pulmonary edema*. A normal sleeping dog breathes 15–25 times per minute; consistently above 30 breaths/min warrants immediate veterinary contact
- Mild exercise intolerance or reluctance to play
- Occasional dry or soft cough, especially at night or after exercise
- Slightly reduced appetite or restlessness at night
The ACVIM 2019 Consensus Guidelines recommend that owners of dogs in Stage B2 MMVD monitor resting respiratory rate at home daily using a stopwatch or a dedicated app (several are available). This simple, free monitoring tool has been shown to detect early CHF decompensation before respiratory distress becomes obvious.
Moderate to Severe Signs (acute decompensation)
- Persistent cough — often moist, productive, and frequent
- Rapid or labored breathing (dyspnea) — increased effort, open-mouth breathing in dogs is always abnormal
- Orthopnea: inability to lie down comfortably; dog prefers to sit or stand upright
- Cyanotic mucous membranes (blue-gray gums) — a true emergency
- Profound exercise intolerance: collapses or stops after minimal activity
- Abdominal distension (right-sided CHF) from ascites
- Syncope (fainting) — brief loss of consciousness, often from arrhythmia or severe low output
- Weakness, weight loss, muscle wasting (cardiac cachexia) in chronic disease
What to Watch for at Home — Owner Action Guide
- Count resting breaths for 60 seconds while your dog is asleep (not after exercise). Do this at the same time daily.
- If resting rate consistently exceeds 30 breaths/minute: call your veterinarian *today*
- If your dog is open-mouth breathing, blue-gummed, or cannot breathe comfortably at rest: this is an emergency — go to a veterinary emergency clinic immediately
- Keep a simple daily log with date, time, and respiratory rate
- Note any changes in cough frequency, appetite, activity level, or abdominal girth
How Veterinarians Diagnose CHF
Diagnosing CHF requires integrating clinical findings with imaging and laboratory data. No single test is definitive; the diagnosis is made from the whole picture.
Physical Examination
- Auscultation: A cardiac murmur (most commonly mitral or tricuspid regurgitation) is present in MMVD and many other cardiac diseases. Murmur grade (I–VI/VI) correlates roughly but imperfectly with disease severity. Muffled heart sounds suggest pericardial effusion or pleural fluid.
- Increased respiratory rate and effort
- Crackles (pulmonary edema) on lung auscultation
- Jugular venous distension, ascites, and peripheral edema (right-sided CHF)
Chest Radiographs (Thoracic X-Rays)
- Heart size (vertebral heart score, VHS)
- Left atrial size — a key predictor of CHF risk in MMVD
- Pulmonary vein and artery caliber
- Pulmonary edema pattern (interstitial → alveolar infiltrates)
- Pleural effusion
Echocardiography (Cardiac Ultrasound)
- Valve structure and regurgitation severity (Doppler)
- Ventricular and atrial dimensions (to track enlargement over time)
- Myocardial contractility (fractional shortening, ejection fraction)
- Pericardial effusion
For MMVD, the ACVIM guidelines define the threshold for initiating medical treatment: left atrial-to-aortic ratio (LA:Ao) ≥ 1.6 on echocardiography and/or VHS > 10.5 on radiographs.
Biomarkers
- NT-proBNP (N-terminal pro-B-type natriuretic peptide): Released by stretched cardiac muscle cells. Elevated levels strongly correlate with cardiac disease severity and help distinguish cardiac from non-cardiac causes of respiratory signs. Useful as a screening test and for monitoring.
- Cardiac troponin I (cTnI): Elevated with myocardial injury; useful for detecting DCM and monitoring disease progression.
Electrocardiogram (ECG) Identifies arrhythmias (atrial fibrillation is common in large-breed DCM and late-stage MMVD). 24-hour Holter monitoring is the standard for Dobermans and Boxers, in which ventricular arrhythmias may be the first manifestation of occult DCM.
Blood Pressure Systemic hypertension can worsen cardiac disease and is checked in all cardiac patients. Renal function (BUN, creatinine, SDMA) and electrolytes are essential before and during diuretic therapy.

Treatment: Medications and Monitoring
CHF management has transformed dramatically in the past decade. Several landmark clinical trials — particularly QUEST (2019) and EPIC (2016) — now guide treatment decisions with strong evidence.
Stage B2 MMVD: Pre-CHF Prevention
The EPIC trial demonstrated that pimobendan (Vetmedin®), started before the onset of CHF in dogs with enlarged hearts (LA:Ao ≥ 1.6 or VHS > 10.5), delayed the onset of CHF by a median of 15 months compared to placebo. This was a landmark finding: it means that at-risk dogs should be screened with echocardiography at their annual wellness visits, and treatment should begin before symptoms appear.
Stage C CHF: Active Congestive Failure
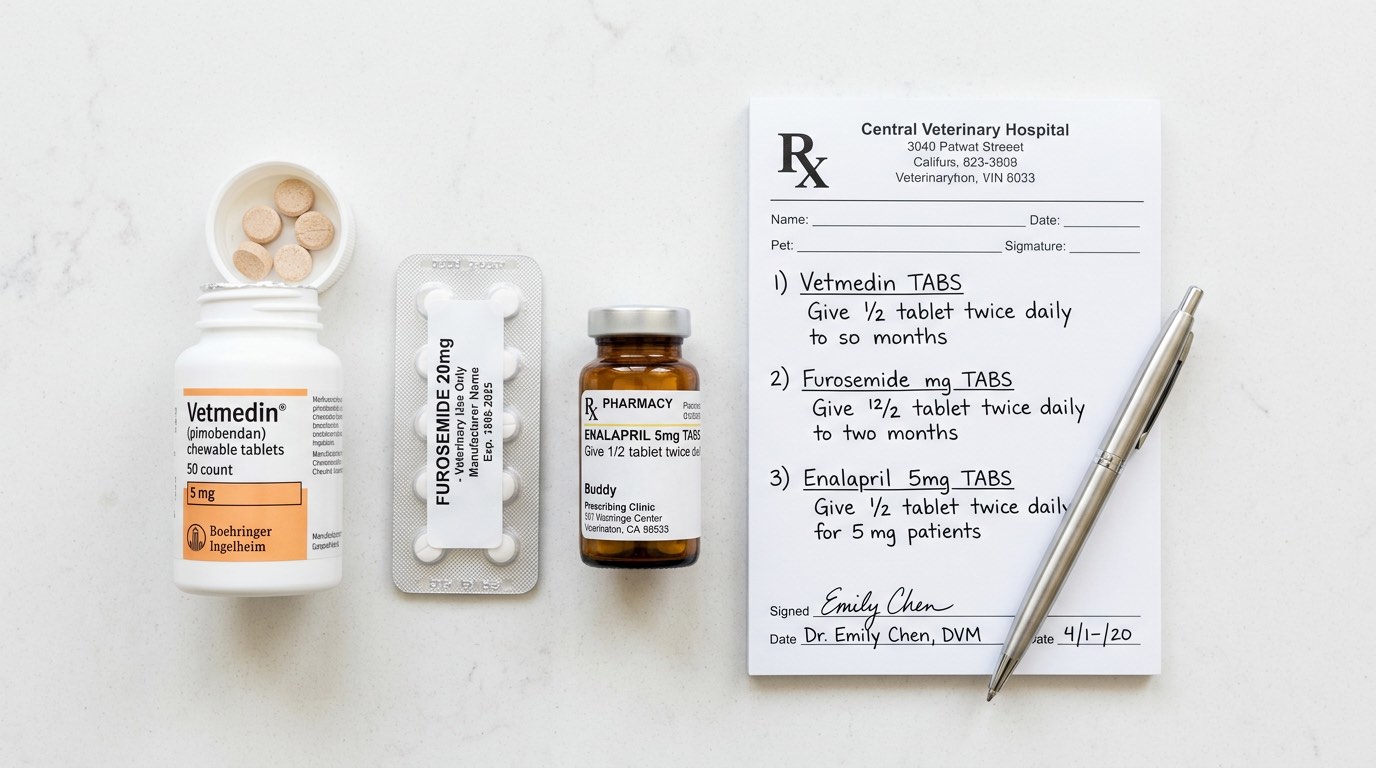
Once CHF is diagnosed, the cornerstone three-drug protocol is:
- Furosemide (Lasix®) — a loop diuretic that removes excess fluid from the lungs and body. Typically started at 1–2 mg/kg every 12 hours and titrated based on response and kidney function monitoring. Without furosemide, acute CHF is fatal.
- Pimobendan (Vetmedin®) — an inodilator that simultaneously increases cardiac contractility (positive inotrope) and reduces cardiac afterload (vasodilator). The QUEST trial in MMVD showed pimobendan significantly extended survival compared to benazepril.
- An RAAS inhibitor — typically an ACE inhibitor such as enalapril or benazepril at 0.25–0.5 mg/kg every 12 hours. Reduces angiotensin II and aldosterone, decreasing fluid retention and cardiac remodeling. In refractory cases, spironolactone (an aldosterone antagonist) is added.
Additional Medications by Situation
- Digoxin: For dogs with atrial fibrillation; helps control ventricular rate
- Diltiazem: Rate control in atrial fibrillation
- Sotalol or mexiletine: Management of ventricular arrhythmias (especially in Boxers and Dobermans)
- Sildenafil (Viagra®): For pulmonary hypertension complicating right-sided CHF
- Taurine supplementation: For breeds or diet-associated DCM cases where taurine deficiency is suspected or confirmed
Monitoring Schedule
Dogs in Stage C CHF typically require:
- Recheck at 7–14 days after initiating or changing medications (assess kidney values, electrolytes, chest radiographs, respiratory rate)
- Stable patients every 3–6 months with bloodwork, radiographs, and echocardiogram
- Owner home monitoring of resting respiratory rate daily
Acute Decompensation (Emergency Management)
- Oxygen supplementation (ideally in an oxygen cage at 40–60% FiO₂)
- Furosemide administered IV or IM at 2–4 mg/kg for rapid diuresis
- Nitroglycerin paste or IV nitroprusside for severe pulmonary edema (venodilation)
- Thoracocentesis for clinically significant pleural effusion
- Strict cage rest during stabilization
Nutrition, Exercise, and Home Management
Medical management of CHF is only one component of comprehensive care. Nutrition and lifestyle modifications significantly affect quality of life and disease progression.
Sodium Restriction
Sodium promotes fluid retention through renal mechanisms. While severe sodium restriction is rarely needed in early CHF (and can actually worsen RAAS activation if too aggressive), moderate restriction is recommended for dogs in Stage C–D. This means avoiding high-sodium human foods, processed treats, and table scraps. Many commercial therapeutic cardiac diets (e.g., Hill's h/d, Royal Canin Cardiac) provide appropriate sodium levels with palatability maintained.
Important: Never feed salty human foods, deli meats, cheese, or snack foods to a dog with CHF.
Maintaining Lean Body Weight
Both obesity and cachexia (muscle wasting) worsen outcomes. Cardiac cachexia — progressive muscle loss in dogs with advanced CHF — results from cytokine-mediated catabolism, reduced appetite, and poor nutrient absorption. If your dog is losing weight, work with your veterinarian on calorie-dense, protein-rich diets (prescription or otherwise) to maintain muscle mass.
Omega-3 Fatty Acids
Fish oil supplementation (EPA + DHA, 40 mg/kg/day combined) has evidence for modest anti-inflammatory and anti-cachexia benefits in dogs with CHF. It also has mild antiarrhythmic properties. Use pharmaceutical-grade fish oil supplements formulated for pets or humans and verify dose with your veterinarian.
Exercise
Dogs with well-compensated CHF benefit from gentle, low-impact exercise — leash walks are appropriate. Avoid strenuous runs, off-leash play with other dogs, and activities requiring sustained aerobic effort. The goal is to maintain muscle tone and mobility without stressing the heart.
As CHF advances, activity will self-limit. Follow your dog's cues: if they want to stop, stop.
Stress Minimization
Stress is profoundly detrimental in cardiac patients — catecholamine release increases heart rate and contractile demand. Minimize travel, changes in routine, and situations that cause anxiety. Discuss anti-anxiety medications with your veterinarian if your dog is prone to stress reactions.
Water Access
Always provide free access to fresh water. Dogs on furosemide lose water through increased urination; dehydration and electrolyte imbalances (particularly hypokalemia) are real risks. If your dog is drinking excessively or very little, report this promptly.
Prognosis, Quality of Life, and When to Seek Help
CHF is a manageable but progressive condition. Prognosis varies considerably based on underlying cause, stage at diagnosis, and response to treatment.
MMVD Prognosis
- Dogs with MMVD in Stage C have a median survival of 9–12 months from the onset of CHF with standard triple therapy
- Pimobendan addition improves median survival to 18–24 months in responding dogs
- Individual variation is high — some dogs live 3+ years with excellent management
DCM Prognosis
- DCM generally carries a poorer prognosis than MMVD, particularly in Dobermans
- Median survival after CHF diagnosis: 6–9 months in Dobermans; somewhat longer in other breeds
- Occult DCM (pre-CHF) with pimobendan initiation: delays CHF by 6–9 months (PROTECT study)
Refractory Stage D CHF
When CHF becomes resistant to standard triple therapy, options include:
- Increasing furosemide dose
- Adding torsemide (a more potent loop diuretic) or spironolactone
- Adding hydrochlorothiazide (a thiazide diuretic) for additive effect
- Frequent thoracocentesis for recurrent pleural effusion
- Discussion of hospice care and quality-of-life assessment
Quality of Life Assessment
The HHHHHMM scale (Hurt, Hunger, Hydration, Hygiene, Happiness, Mobility, More good days than bad) adapted for cardiac patients is a practical tool. Schedule an honest conversation with your veterinarian about quality of life when:
- Resting respiratory rate cannot be controlled below 30 breaths/min despite medication adjustments
- Your dog cannot sleep comfortably
- Appetite is severely reduced and weight loss is significant
- The dog appears distressed, anxious, or unable to enjoy any activities
CHF is one condition where close partnership with your veterinary team — particularly a board-certified cardiologist if referral is possible — makes a measurable difference in both length and quality of life.

Frequently Asked Questions
Can a dog live a normal life with CHF?
Many dogs with CHF enjoy good quality of life for 1–2+ years with appropriate medical management. The key is early diagnosis, consistent medication, home respiratory rate monitoring, and regular veterinary follow-up. Most dogs can enjoy gentle activity and a comfortable daily routine with well-controlled CHF.
What does CHF cough sound like in dogs?
A CHF-related cough is often soft, moist, and most frequent at night or after rest. It can sound like gagging or clearing the throat. In contrast to kennel cough (which is harsh and honking), cardiac cough is typically not productive and worsens with lying down as fluid redistributes. Any new or worsening cough in a dog with a known heart murmur warrants veterinary evaluation.
How long can a dog live with congestive heart failure?
Median survival after CHF diagnosis with standard triple therapy is approximately 9–18 months for MMVD, though significant individual variation exists — some dogs live 3+ years. DCM generally carries a shorter prognosis. Survival is strongly influenced by how early treatment begins, how well medications are tolerated, and the owner's ability to monitor and adjust care.
Is pimobendan expensive?
Pimobendan (brand: Vetmedin®) costs approximately $1.50–$3.00 per tablet at veterinary pharmacies, and dosing is weight-based. For a medium-sized dog, monthly costs typically range from $60–$120. Compounded versions are available but should be used cautiously, as bioavailability can vary. Discuss cost management options with your veterinarian, including Canadian pharmacies or veterinary prescription programs.
Should all small dogs be screened for heart disease?
The ACVIM recommends annual cardiac auscultation for all dogs after age 5, with echocardiography for dogs with documented murmurs and breeds at high risk (especially Cavaliers). Cavalier King Charles Spaniels have a specific breed health screening protocol through the Cavalier Health organization. Early detection of enlargement triggers pimobendan therapy, which meaningfully extends the time before CHF develops.
References
- Boswood A, et al. "Effect of Pimobendan in Dogs with Preclinical Myxomatous Mitral Valve Disease and Cardiomegaly: The EPIC Study." Journal of Veterinary Internal Medicine, 2016;30(6):1765–1779.
- Keene BW, et al. "ACVIM Consensus Guidelines for the Diagnosis and Treatment of Myxomatous Mitral Valve Disease in Dogs." Journal of Veterinary Internal Medicine, 2019;33(3):1127–1140.
- Häggström J, et al. "Effect of Pimobendan or Benazepril Hydrochloride on Survival Times in Dogs with Congestive Heart Failure Caused by Naturally Occurring Myxomatous Mitral Valve Disease: The QUEST Study." Journal of Veterinary Internal Medicine, 2008.
- Oyama MA. "Using Cardiac Biomarkers in Veterinary Practice." Veterinary Clinics of North America: Small Animal Practice, 2013.
- Freeman LM. "Cachexia and Sarcopenia: Emerging Syndromes of Importance in Dogs and Cats." Journal of Veterinary Internal Medicine, 2012.