
Quick Answer
A thorough guide to Addison's disease (hypoadrenocorticism) in dogs — a condition where the adrenal glands fail to produce sufficient cortisol and/or aldosterone. Covers the two forms (typical vs atypical), why it's called the great pretender, the acute Addisonian crisis, ACTH stimulation testing, and lifelong management with DOCP and/or prednisone.
Key Takeaways
- ✓Addison's disease is called the 'great pretender' because its vague, waxing-and-waning signs mimic many other conditions — often for months before diagnosis
- ✓The classic lab clue is a low sodium:potassium ratio (<27) on bloodwork — this should prompt an ACTH stimulation test immediately
- ✓An Addisonian crisis is a life-threatening emergency requiring immediate IV fluids, dexamethasone, and cardiac monitoring
- ✓DOCP injections (every 25–28 days) plus daily low-dose prednisone replace the missing hormones and allow normal quality of life
- ✓Stress dosing (tripling prednisone) during illness, surgery, or stressful events is critical — Addisonian dogs cannot produce extra cortisol on demand
What Is Addison's Disease?
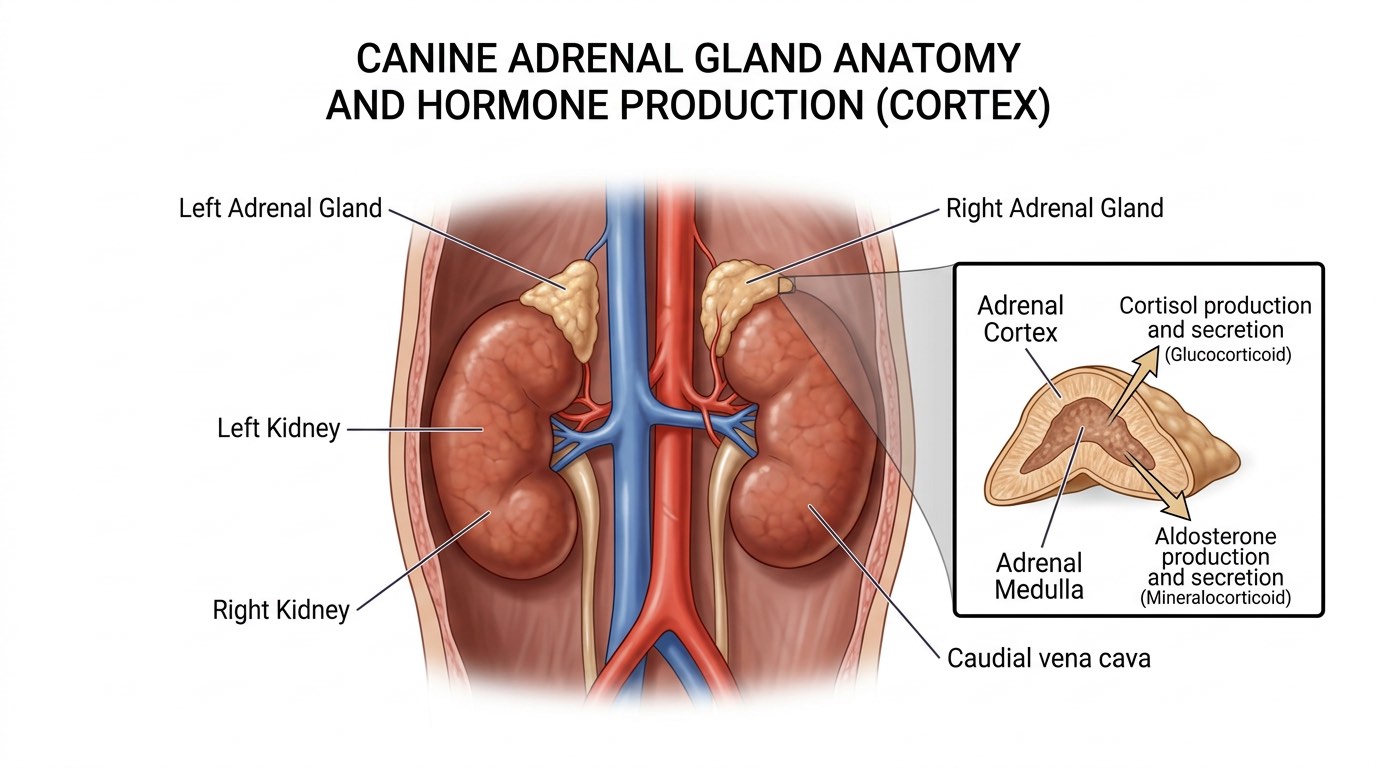
Addison's disease — medically termed hypoadrenocorticism — occurs when the adrenal glands, two small glands positioned adjacent to the kidneys, fail to produce sufficient quantities of their essential hormones. The adrenal cortex normally produces two critical classes of hormones: glucocorticoids (primarily cortisol), which regulate metabolism, stress response, blood glucose, and immune function; and mineralocorticoids (primarily aldosterone), which regulate sodium and potassium balance and, by extension, blood pressure and fluid balance.
In most affected dogs (typical hypoadrenocorticism), both hormone systems fail simultaneously. The consequences are broad and serious: without cortisol, the body cannot mount an appropriate stress response and blood glucose regulation suffers. Without aldosterone, sodium is lost and potassium accumulates — eventually reaching cardiac-toxic levels. This combination of cortisol and aldosterone deficiency produces a diverse array of vague, waxing-and-waning clinical signs that mimic many other conditions, earning Addison's disease its nickname: the great pretender.
Atypical hypoadrenocorticism involves only glucocorticoid deficiency with intact mineralocorticoid function — affected dogs lack the classic electrolyte abnormalities and the condition can be even harder to identify. The disease can be primary (immune-mediated destruction of the adrenal cortex — the most common cause) or secondary (failure of pituitary ACTH stimulation of the adrenal glands, often from abrupt steroid withdrawal). Young to middle-aged female dogs are most commonly affected, and certain breeds carry higher risk: Standard Poodles, Portuguese Water Dogs, Bearded Collies, Great Danes, and West Highland White Terriers.
Signs: The Great Pretender in Action
The clinical signs of Addison's disease are notoriously vague and intermittent in the early and chronic phases, which is why the average time from onset of symptoms to diagnosis can be months to years. Dogs typically present with episodic weakness or collapse, lethargy, vomiting, diarrhea, decreased appetite, weight loss, and shaking. These episodes often occur during stressful events — a car ride, a grooming appointment, a visit from strangers — because the dog cannot mount a normal cortisol stress response.
Owners frequently describe a dog who has 'good days and bad days' — improving temporarily with supportive care (IV fluids, a steroid injection) and then relapsing. This pattern of improvement followed by relapse is a classic tell for Addison's disease, and a dog that responds dramatically to a single dose of dexamethasone warrants Addison's disease workup. The classic laboratory finding is the combination of hyponatremia (low sodium) and hyperkalemia (high potassium) producing a sodium:potassium ratio below 27 — a finding that, when identified on routine bloodwork, should immediately prompt ACTH stimulation testing.
Atypical Addison's disease, lacking the electrolyte abnormalities, is even more challenging and may be diagnosed only after ruling out many other causes of waxing-and-waning GI and constitutional signs. Dogs with atypical disease may have normal sodium:potassium ratios and the only way to diagnose them is the ACTH stimulation test.

Addisonian Crisis and Diagnosis
An Addisonian crisis is a life-threatening acute adrenal emergency in which an affected dog decompensates suddenly, presenting in shock with profound weakness or collapse, severe vomiting, bradycardia (slow heart rate from hyperkalemia-induced cardiac conduction disturbances), and cardiovascular instability. Without immediate aggressive treatment — IV fluid resuscitation with normal saline, dextrose if hypoglycemic, a fast-acting glucocorticoid (dexamethasone sodium phosphate), and cardiac monitoring — affected dogs can die within hours.
The diagnosis of Addison's disease is confirmed by the ACTH (adrenocorticotropic hormone) stimulation test — the gold standard. A baseline cortisol level is measured, synthetic ACTH (cosyntropin) is administered, and cortisol is re-measured 60 minutes later. Normal dogs show a significant cortisol rise in response to ACTH stimulation. Addisonian dogs show a flat, blunted response — both baseline and post-ACTH cortisol levels are abnormally low. Dexamethasone is used during the crisis because it does not interfere with the cortisol assay, allowing the ACTH stimulation test to be performed simultaneously with treatment.
Additional diagnostics often reveal a classic 'reverse stress leukogram' on CBC (lymphocytosis and eosinophilia, the opposite of the expected stress response), along with the hyponatremia/hyperkalemia pattern and sometimes elevated BUN from poor renal perfusion. Abdominal ultrasound typically shows very small (atrophied) adrenal glands, a supportive though not definitive finding.

Lifelong Management: DOCP and Prednisone
Addison's disease requires lifelong hormone replacement therapy, but with appropriate management, affected dogs live normal, comfortable, full-length lives. The treatment varies between typical and atypical forms.
For typical hypoadrenocorticism (both mineralocorticoid and glucocorticoid deficiency), mineralocorticoid replacement is the cornerstone. DOCP (desoxycorticosterone pivalate, brand name Percorten-V) is a long-acting injectable mineralocorticoid given every 25–28 days. It replaces the aldosterone function, normalizing sodium and potassium balance and preventing the life-threatening electrolyte emergencies. Fludrocortisone acetate (Florinef) is an oral daily alternative that provides both mineralocorticoid and some glucocorticoid activity. Alongside mineralocorticoid replacement, low-dose prednisone is given daily to replace cortisol — typically at physiological doses (0.1–0.2 mg/kg/day), not immunosuppressive doses.
For atypical hypoadrenocorticism, only daily prednisone is needed initially — however, many atypical dogs eventually develop electrolyte abnormalities over time and transition to typical disease, requiring mineralocorticoid supplementation later. During stressful events (illness, surgery, travel, boarding), all Addisonian dogs require stress dosing — temporarily tripling the prednisone dose to compensate for the inability to increase cortisol naturally. Owners should always carry injectable dexamethasone and be coached on emergency protocols. Electrolytes and ACTH stimulation tests are rechecked every 3–6 months to fine-tune DOCP dosing.

Frequently Asked Questions
What are the early signs of Addison's disease in dogs?
Early signs are frustratingly nonspecific: episodic lethargy, vomiting, decreased appetite, weakness, and occasional shaking — especially during or after stressful events. Dogs often seem to partially recover with supportive care, only to relapse. If your dog has repeated episodes of GI upset and weakness that seem stress-related and improves with IV fluids and steroids, Addison's disease should be on the differential list.
How is Addison's disease diagnosed?
The gold standard diagnostic test is the ACTH stimulation test. A baseline blood cortisol is measured, synthetic ACTH is injected, and cortisol is remeasured 60 minutes later. A blunted, low cortisol response confirms Addison's disease. Supporting findings include low sodium, high potassium (Na:K ratio below 27), atrophied adrenal glands on ultrasound, and an abnormal CBC pattern.
What is an Addisonian crisis?
An Addisonian crisis is a life-threatening acute adrenal emergency characterized by sudden collapse, profound weakness, severe vomiting, slow heart rate (from high potassium affecting the heart), and cardiovascular shock. It requires immediate emergency veterinary treatment with IV fluids, injectable glucocorticoids (dexamethasone), and cardiac monitoring. It can be fatal within hours without treatment.
Can dogs with Addison's disease live a normal life?
Yes — with proper hormone replacement therapy, Addisonian dogs typically live full, normal lives with an excellent quality of life and normal lifespan. The key requirements are consistent medication (monthly DOCP injections and daily prednisone), routine monitoring of electrolytes every 3–6 months, stress dosing during illness or stressful events, and having emergency dexamethasone available at home.
What is stress dosing and when is it needed?
Stress dosing means temporarily increasing the daily prednisone dose (typically tripling it) during periods of physiological or psychological stress — illness, surgery, hospitalization, travel, boarding, or any event causing significant anxiety. Normal dogs produce extra cortisol during stress; Addisonian dogs cannot. Without stress dosing, affected dogs risk decompensating into an Addisonian crisis. Your veterinarian will advise on the specific dosing protocol for your dog.
References
- Feldman EC, Nelson RW. Hypoadrenocorticism. Canine and Feline Endocrinology and Reproduction. 3rd ed. 2004.
- Klein SC, Peterson ME. Canine hypoadrenocorticism: Part I. Can Vet J. 2010.
- Scott-Moncrieff JC. Hypoadrenocorticism. Textbook of Veterinary Internal Medicine. 7th ed. 2010.
- Lifton SJ, et al. Hypoadrenocorticism caused by ACTH deficiency in the dog. JAVMA. 1996.